Jeremy David Engels was kind enough to join us on the Becoming a True Human podcast! Listen in for an enlightening discussion of a revised Declaration of Independence – A Declaration of Interdependence!
Jeremy David Engels discusses his new book, On Mindful Democracy with Dave Kopacz and Chris Smith. We start by asking him about the nature of the “true human” and “true democracy.”
In the book he defines true democracy as “working together to care for each other and the life we share,” (4).
The book is divided into three parts, recognizing our common ground, walking the path of interdependence in community, and practicing democracy with hands and heart.
Jeremy has drafted a new interpretation of the Declaration of Independence as the Declaration of Interdependence.
Throughout the book and our discussion, he draws on Thich Nhat Hanh’s concept of interbeing as a foundation for our common ground of mindful interdependence – and he draws on Martin Luther King Jr.’s concept of the beloved community as a model of mindful working together to foster true human connection.
Jeremy elaborates the concepts of “enemyship” (viewing relationships as us vs them, and competitive and conflictual – the opposite of interbeing) and mindful deliberation as a modality of working with tensions within the individual and within communities. He tells us that “there is no way to democracy, democracy is the way,” (103).
We discuss a great idea of bringing together various thinkers on contemplative forms of democracy, such as mindful democracy, spiritual democracy, and inner democracy – into The Varieties of Democratic Experience (with a nod to William James).
Jeremy closes our discussion with a poem from his book, entitled Hope (p. 155):
Hope
Snow melts from a tree branch Someday soon it will be a cloud And rain will fall on new leaves
There is spring in winter And winter in spring Take heart
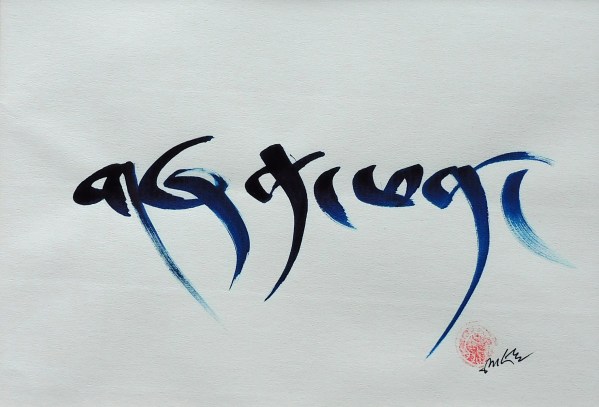
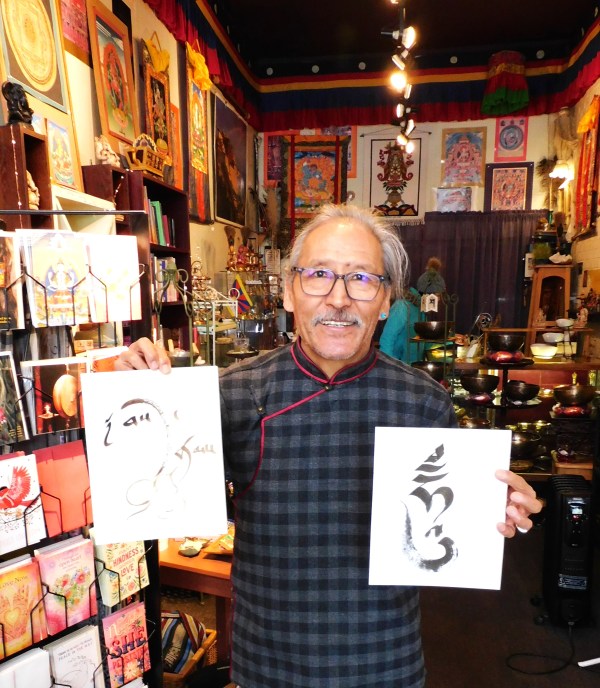
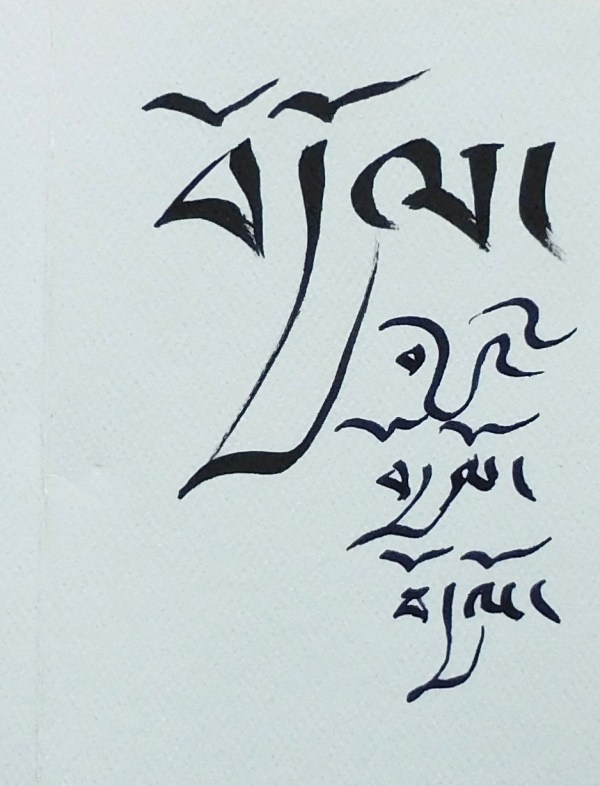
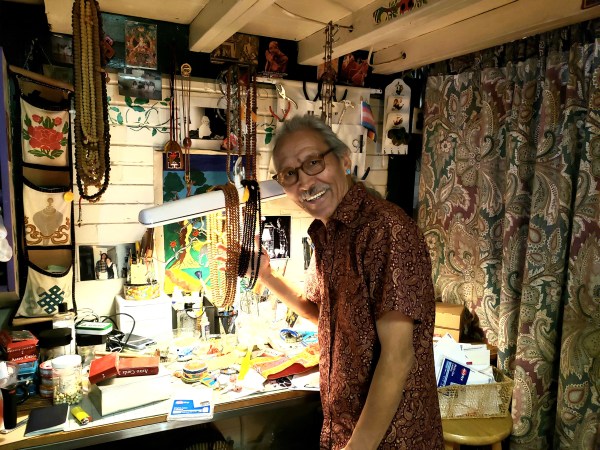
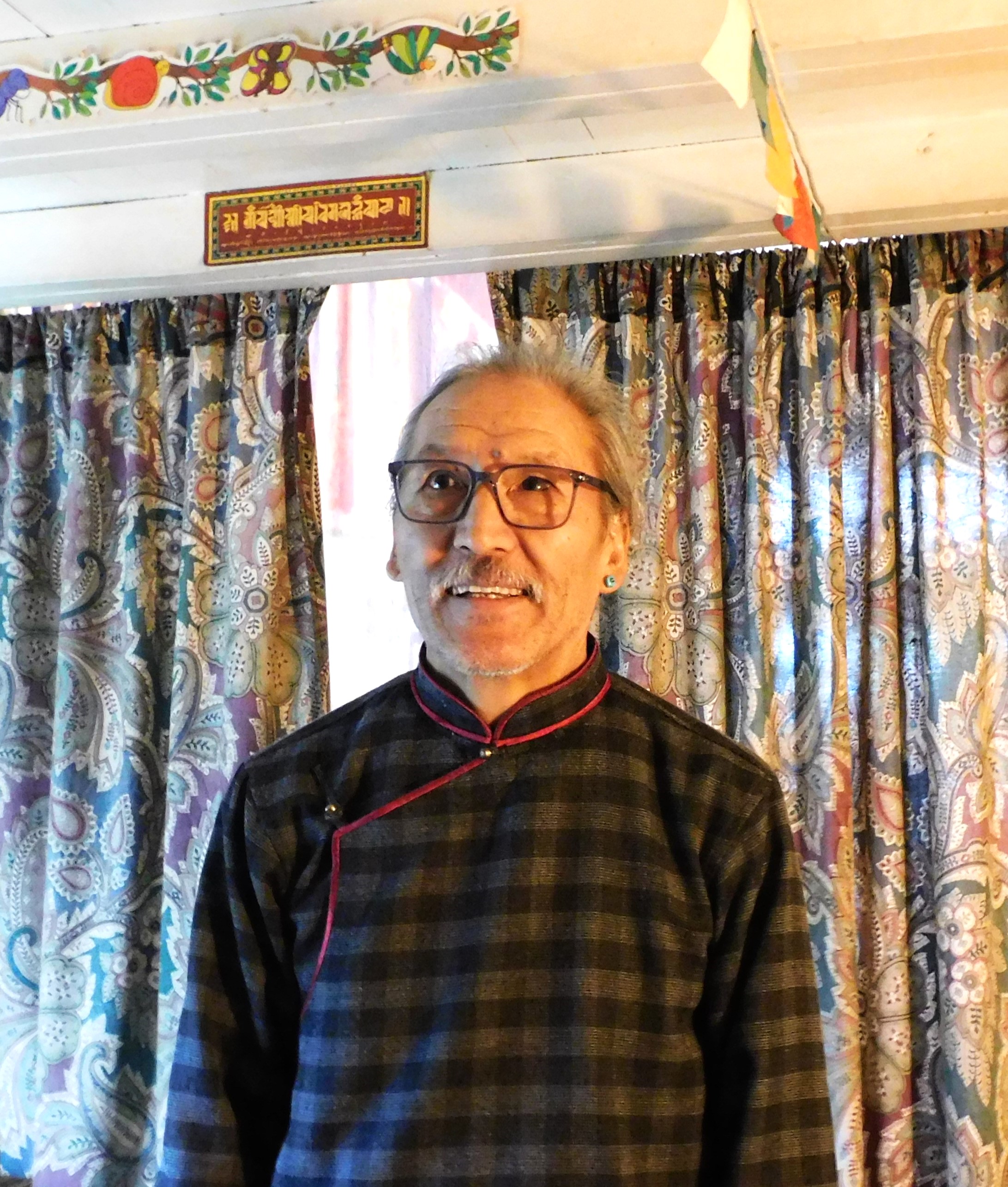
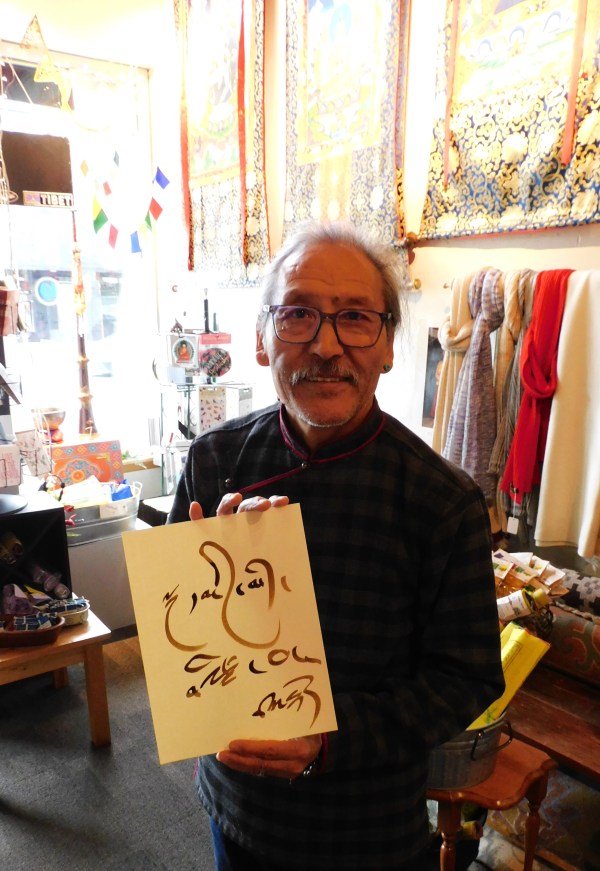
Rigdzin is the proprieter of Pema Kharpo, a shop selling imported Tibetan and Asian good, in the Greenwood neighborhood of Seattle. This was my go to place when I was looking for gifts for others, or a mala for myself. The place is good medicine. Rigdzin would often give me something for health or protection if I was feeling under the weather or traveling. We moved away from Seattle to Madison, Wisconsin in 2025 and I miss my conversations with Rigdzin, but I am finally getting this interview we did in 2024 posted! Rigdzin’s life story is so fascinating, born in Tibet, raised in exile in Dharamshala, meeting with the Dalai Lama on his visits to the Tibetan school, traveling to the US, working in restaurants and starting an import business on the side, serving as an interpreter for Tibetan monks on tours of the US, and now running Pema Kharpo and helping people connect to Tibetan spirituality. We will intersperse his calligraphy art throughout the interview.
David R. Kopacz: As I have spoken with you over the years I’ve been in Seattle, it seems you’ve had many roles in your life. Could you start at the beginning and tell me a little about your childhood and your time growing up in Tibet and then in exile in India after the Chinese invasion of Tibet in 1959?
TIBET TO DHARAMSHALA
Rigdzin: I was one of those who were forced from their country and forced to live in another country. This is part of my role and life starting with unfairness—the opposite of peace. My parents went to India when I was two. So, I experienced, for example, living in a tent, as a concentration camp, so to say, but under the great open heart from India, at that time. We didn’t have any other countries’ support. Only India acknowledged that Dalai Lama can come in exile to Dharmshala. My role was like a child who was victimized by war and extreme poverty.
At a very young age, I was exposed to many, many different situations. I speak many languages, that’s one advantage. Another thing, I also really understand others’ pain. And the greatest blessing was the Dalai Lama’s teachings and Buddhism. From the very beginning, Dali Lama has taught about compassion, all the time, compassion. In Tibetan, this is nying-je. The literal word, nying means “heart,” je means “mighty.” Our heart is mighty, because you can understand others’ pain and see that anger and hatred causes so much suffering. The entire philosophy of Dalai Lama is always putting the other as more important than you. That is the philosophy I was brought up with.
DRK: So, you say that even though there were hardships of being in exile, and being a child of war, and being in extreme poverty, there were things that you saw as gifts like learning many languages and being able to see others’ suffering.
Rigdzin: Also, it was because of His Holiness Dalai Lama’s gentleness and love and his unwavering non-violence that actually gave us more strength, because the truth is greater than the force of hatred or bullying.
Rigdzin: Yes. I sometimes jokingly call my parents, “Dalai heads.” You know, you have a “dead head,” right? Who follows around the band the Grateful Dead? So, I remember my parents like that, following around the Dalai Lama wherever he went or wherever he sent them.
My father was a businessman. He had donkeys and ponies and horses and yaks. He would bring things from Tibet, and then he would bring back things from India. See, he already knew the route to India. So, when he escaped the Chinese invasion, sometimes we were one day apart from His Holiness Dalai Lama and sometimes one week apart on the journey to India. So, His Holiness first went to Arunachal Pradesh and we were already there.
I remember, as a child, since I was maybe three years old, I stayed in a tent. So even today, sometimes my wife takes me camping. When the weather is bad, I get nervous. Because for me, it is no fun living in a tent, ha ha! Especially when we had a tent that was Indian military surplus—they don’t have a floor!
Dali Lama left Tibet on March 17, 1959, after sometime he arrived in Dharamshala in April, 1960. My parents were the first ones who built the Dalai Lama’s new residence. And after they built that, our group was sent to different South India locations, because His Holiness’ whole idea was the future of Tibet.
All the kids were given some form of school, hostel school, boarding school, so that parents can go and make a living and the kids can learn Tibetan. My parents followed everywhere His Holiness Dalai Lama went or directed. They were 100% dedicated to His Holiness. They were unwavering, trusting the guidance of His Holiness Dalai Lama, for the good of their kids and themselves, as well as the people still inside Tibet who didn’t have a voice.
DRK: So, His Holiness was thinking of the future of Tibet and your future.
DRK: You’ve told me you were able to have audiences with His Holiness. Could you say more about what those meetings were like?
Rigdzin: See, after we moved to Dharamshala, I look back and think that was one of the most fortunate things that happened, because we got to see His Holiness Dalai Lama every other week. And we were all kids, but sometimes we were fifty, and sometimes we were two hundred. We would go to see His Holiness in his first residence, which was, actually, an old British summer house. I still remember, that his windows were broken, the glass was broken. So, we flattened American aid or Western aid, oil, cooking oil cans. They come in twenty-five gallon cans, the square ones. So, after the oil is done, we cut them, flatten them, and put a color on them. So, we made windows out of the metal cans. And His Holiness, maybe at that time was twenty-seven or twenty-eight years old
We were kids from maybe five to eleven years old. We all lined up and were excited to see His Holiness and he gave us advice. I still remember his advice at the time, according to our age and capacity, he said “I want you guys to be like a flower in the wild, not like in a manmade garden that can easily whither each season.”
At that time we didn’t know much about sanitation. We didn’t have hot water, no towel, very little, maybe one towel for ten kids. So, he said, “If you wash your face nicely, if you wipe your nose good, that also will help for Tibet, because people will say, ‘Look at that clean, smiling face, that kid is a Tibetan.’” I never forgot that was something that I could do. And always he told us we are fortunate and to be proud, because we are the children of compassion, tolerance, and good manners. Those are the things he liked to talk about. Then he always said, “Take care of each other.” Basically, encouraging compassion to everybody, even to the insects. As kids we grew up with those words and ideas which are really the blessings!
DRK: It sounds like he inspired you to think of yourself almost like an ambassador or emissary for Tibet. Anything else about those years and the experience of seeing the Dalai Lama?
Rigdzin: Yes, from the beginning, He saw each one of us having a profound responsibility for the future of Tibet. Nowadays, we are getting a deeper understanding of his vision, basically, perseverance of the message of truth and compassion, and that we are all interdependent. If we inflict harm to others, it has no end, it only gets worse. Our greater responsibility is the understanding that everyone equally wants happiness, but out of their own shortcomings, they inflict bullying and harming on others. But, actually, everyone is also exactly like me—who wants to be happy, who wants to be respected. So, I understand now the bigger and deeper meaning of why he has always taught non-violence. At that time, we were just kids, right? We just wanted to be mad with China, but His Holiness always says peace is the only possibility.
DRK: How did you end up coming to the United States?
COMING TO THE UNITED STATES
Rigdzin: I met a gentleman on an Indian street; I was selling clothes. I called it my Pema Kharpo [shop] on the street! Ha ha ha! I didn’t know in the future I would own an actual shop. Then I met this wonderful, tall, well-built Westerner, but wearing completely, torn clothes—he looked like a hippie. He looked very strong and he had a lot of cameras. He sat next to me, and he talked to me, because I was trying to read the newspaper. This happened to be an English newspaper. I didn’t know how to read very well. It was more like I wanted to have the image of reading, ha ha ha! He said, “Do you read English?” and then we talked and he said, “You are pretty good. Do you want to go to school?” I said, “I have no money.” “So you want to go to college?” “Yeah!” Then he said, “I will pay for your college fee.” So that’s how it happened. And he asked, “How much it will cost.” And I said, “10,000 rupees,” which was a lot of money at that time. $1 was about eleven rupees. Right now, it is 83 rupees for a dollar. So, he really gave me cash, ₹10,000.
So, I went to New Delhi, and I joined vocational college. And then, many years later, I also got a part-time job in a restaurant. And then two women from Olympia, Washington came in the restaurant looking for someone and asked me, “Do you know Rigdizin?” “Yeah,” I say, “I’m Rigdzin! And then they say, “We’re Chris’ friends.” And then I realized that he sent them to me because I could show them around. So, then I helped these two ladies as a guide. Then they asked me if I wanted to come to America and see what America looked like. They were very curious because one of the ladies said that she remembered ten lifetimes of her past life. And she describes scenery and regions in India and so we go—and they are really there! She said her family thinks she’s crazy. But that’s not crazy for me. So, that’s how we become friends. They invited me to come to see America. So, I came first to Olympia, Washington, and I liked it. Then I went back to India, to bring back more goods. I was lucky to get a visa, a business visa, legally. So, within one year, I could come and go. I went back to India and then I came back to the US and then stayed right here in Seattle.
PEMA KHARPO: WHITE LOTUS
DRK: What did you do in the States then? Did you continue your shop, Pema Kharpo?
Rigdzin: Slowly, slowly, I started to bring my children here. For a few years, I asked for political asylum and then I immediately got a work permit. I worked some but mostly I explored America. People asked me to come here, come there, and I just went. And this is when I learned not only the language, but how people eat, right? How people fight. How do you use the bathroom. What is your culture and all of that. Then I picked up English very fast. I went to community college to brush up my English. But mostly I worked in a restaurant early on.
Then, the first time I went back to India to see my brothers and sisters, I had a credit card. Always, in the back of my mind, I wanted to do something for my community. So, when I had the credit card, I bought 100 rugs from our village. The Women’s Association, something like that we called it, through handicraft, made handmade carpets. Then in Olympia, I worked full-time as a cook. But every other weekend, sometimes, I would throw a small party and sell rugs out of my friend’s apartment. That’s how I started Pema Kharpo! Ha ha ha!
DRK: What does Pema Kharpo mean?
Rigdzin: White Lotus.
This is not just a flower. It has a lot to do with the Buddhist philosophy. The lotus grows from muddy water, but it does not carry muddiness, it is pure. So, we are all living beings born out of father and mother’s activity and desire. But each individual mind is uncontaminated and always has the possibility of complete awakening or freedom. Just like the lotus is growing muddy water—it is pure, it doesn’t carry that muddiness. My wife, when we first started the business, asked my brother, “Please give us some the Tibetan names of some flowers for the name of the business.” Then my brother said, “Pema Kharpo” So, yeah that’s perfect, ha ha ha! If you see images of the Buddha, they all sit on moon disc and lotus petal.
DRK: So, the shop started as a way to help people back home by selling their goods?
Rigdzin: Yes! This gives me a real joy and platform to express my art and my culture. Nowadays, I’ve been here 28 years, I have a lot of repeat customers. A lot of times, I get people who will ask me more questions than they buy. But I’m never unhappy about and like you said before, I have a responsibility even though I don’t know that much. But as a Tibetan, His Holiness said, “You are representing Tibet.” So, I try my best. When people have a question about Tibet, the diaspora, and Buddhism, I definitely have a little bit more insight than others who haven’t been through what I have been through. So, it gives me joy!
DRK: So, you’re a businessman. But you’re also—I suppose a businessman is a conduit of bringing something from one place to another place—but you’re also a knowledge man. You bringing knowledge from one place to another?
SERVING AS AN INTERPRETER OF THE DHARMA
Rigdzin: Yes. And also, as I’ve polished my English, somehow I became an interpreter for many, many different visiting monks and a lot of political activists. For example, I translated for six or seven political prisoners, some of them are nuns who spent years in Chinese prison. They’re very, very sad stories.
Foremost, there was a one Tibetan monk, who was the most known in worldwide, Palden Gyatso. He wrote a book called Autobiography of a Tibetan Monk. So, I organized lectures at many places that I’d already been before with other Tibetan monks. So, I knew of sponsors in small, small outlets, so I called them and they’re all happy to receive Palden Gyatso and help him spread his words. He spent 33 years in Chinese prison.
During those times, people would ask what they could do for Tibet. I collected people’s addresses, then I went back to India, in my village, and put all these names in a hat. People would pick a name and then they would get a sponsor.
People would ask me, “Can you find me a sponsor?” One time, this lady came to me, crying, because her parents died, and she’s the oldest one in the family and they have other two kids. She asked if I could find her a sponsor so she could go to college, just a two-year college. I was able to find a sponsor for her. After many years, I got a call from Canada. The lady said, “Hey, Rigdzin do you remember me? You helped me go to college. I worked and I took care of my family. Now I’m in Canada!” This joy, right? Ha ha ha! It’s not me. Like you said, I’m a conduit. I don’t have money to give in my pocket.
DRK: Right, but you know how to connect people. How many time have you gone back and forth between the U.S. and India?
Rigdzin: At least eight times. I wish I could go every other year. I just love to see His Holiness. But I try to go whenever His Holiness gives a major teaching, for like 10-15 days at a time. I’d love to go to Dharamshala again, and maybe one more Tibetan New Year! Ha ha ha!
DRK: What year were you born?
Rigdzin: Two years before we escaped the invasion in 1959, I was born in 1957.
Also, as a child, I remember—you said the role, right. Even when I was young, a lot of people would come to ask me about something they could not find, if they lost a cow. I don’t know why they would. Tibetans have a cultural belief, that kids are innocent and pure and know things adults don’t. So, they ask kids questions. So, in that way, I was a little bit like an adult when I was like six or seven years old. I remember one time in our dormitory some kids lost something. Somebody stole it they thought. So as a kid they were asking me. And I said, “Okay, we have to do three prostrations to the picture of Buddha.” And then I said you have to be honest and if you’re not honest, you are going to shit in front of us. And as we did one kid literally shat, I still remember! He acknowledged he took it. So that things like that, see?
What I’m saying is, it is part of our culture. Then after many years in 2007, 48 years in exile for me, I knew I had a sister who is the oldest. My dad told me, when I was born, my sister was 24-25 years old. So, she would remember everything. I always wanted to go to Tibet and find her. And finally, I found her. I was able to meet my sister and she told me where I was born, and who gave me the name, right. So, so exciting! All this lifetime, I didn’t know. I just wanted to see what kind of place I might have been born. Right. So, when I was in Olympia, the newspaper people asked, “Where were you born?” I’d say, “In Tibet.” They would say, “Where in Tibet?” I’d say, “I don’t know, in a cave!” Ha ha ha!
Anyway, in 2007, my sister said, “When you were a kid, whatever you said would come true.” I said, “What do you mean?” She said, that when the Chinese started coming, you said that our uncle would be killed. She told me that I said my uncle would be killed and we would all go far away to live in a tent and not return. She told me I said that, and it all came true. Maybe that is the reason I became an interpreter because I could know things like that.
DRK: An interpreter is a conduit of languages between people.
Rigdzin: My father, and my ancestors, they were all healers. But also, it’s not just my family, the entire Tibetan people are like Native Americans. Especially like, two, three hundred years ago there were a lot of shamanic rituals, and all mountains are sacred, all rivers are sacred, like that. In my village, when I went in 2007, each household has a spirit. And they pray every morning. That’s very shamanic.
DRK: In Tibet, there was the shamanic culture, and then the Hindu culture, and then the Buddhist culture. And all three came together.
Rigdzin: Yes, yes. For Tibet, our earliest religion was called Bon, Bon was all shamanic. And yes, it has the Hindu, and within the Hindu there are many different Hindus right? With us, we are those who pray to snakes in the rivers, who are Naga. Similar like that, like in Kathmandu, all over the backs of the Himalaya there’s a lot of shamans.
DRK: Like Mount Kailash?
Rigdzin: Yes, Kailash was very close to our village, when I went, I could see in the distance Mount Kailash.
DRK: So, you were able to go to Tibet for the first time in 2007?
Rigdzin: First time and last time. It was just before the Olympics, and it was little bit scary because the Chinese asked lots of questions at each checkpoint. I was an interpreter for political activists and it was the same thing that they asked, each check point, if we were political activists. I was getting scared. But luckily, I was smart. I had a gentleman from Seattle, and he’s a big guy like you, and he was with me. They said, “Who is he?” I said he is my brother-in-law. Ha ha ha! He dressed more like military color and his hair was short. I was more confident because he is right next to me. So, I was not that scared. Otherwise, in Tibet, people disappear overnight.
How many Tibetans, for example, have been put in prison overnight? Recently I saw, they’re building a dam, they build many of them, but now what they’re building is a hydraulic dam in the most sacred and important river, the Yangtze River. And what do the monks do? We don’t believe in killing others. So many Tibetans, like 100, and monks, over 30, they self-immolated.
Dalai Lama’s guidance, you know, is about just expressing our pain without causing pain to other. And now, these monks and nuns, the entire village, great monks, great masters, they’re touching the feet of Chinese officers, begging them, please don’t build the dam. They’re begging them, crying the entire village coming like this, “Please don’t do this. That’s all we have.”
So, sometimes I get really mad about international, powerful countries always talking about peace, peace, but people who are walking the peace and talking the peace are left behind. Until people who can terrorize them, then they get attention. So, it is very, very sad and appalling.
In Tibet, if you are born there, you can’t say you were born in Tibet, you have to say you were born in China. When a paper interviews me, when they ask where I was born, they say they can’t write Tibet. I tell them, “I’d rather you write India than China.” That is how unfair it is, not only by force was Tibet taken, but then international communities still fail even to write the name, “Tibet,” on piece of paper. That’s my right. As a human being where I was born, I was born in Tibet. “No, no,” they say, “you should write China.”
So, this is how we give in to bullies and guns. You know, at the gun point they ask who you are. I say, “I’m human.” But no, no, they say, “Say you are a cat!” That’s how we feel right? When we say I’m born in Tibet, but no, we can’t we have to say “China.” That is sometimes very painful.
As a Buddhist, someday, I think maybe those Chinese people, the lucky ones, may be born into a Tibetan family. I know that sounds completely bizarre. But I’m saying, whenever we harm, it is putting a green light to continuous harming each other on earth. You know, we—each individual—you can say it is government, but the government is built by individuals, right? In order to become peace, individually, we really have to understand at a deep level that we are all the same. Whenever we get into the rigidity of me versus you—I’m better, you’re black, you’re white, you’re Asian, you’re Chinese—you’re my enemy. It’s really sad, right? If we really meditatively become open-minded, friends become enemies, and enemies become friend. Same thing in a bigger picture, if the world is one family, we are just burning ourselves.
There will be no end to the war. Sorry, it’s very depressing. But again, being taught about Buddha nature, and immaculateness of our innate mind, if we all really think deeply, it is possible. Like His Holiness says, “One human, one Earth.” We can live more harmoniously and happier and have more luxury than killing each other. It takes more time, more effort to kill and to destroy, then do live as it is. Just, just be, be patient, be respectful of each other.
Everywhere. We are just blaming each other, even the temples, the school shootings. I’m not just talking about America—everywhere—in some part of the world, blaming each other racially, you’re this party, you’re that party. Both are similar people within the country, but now people focus on division. And now this is scary in America, and the world, right?
DRK: With Tibet, from the exile in 1959, it doesn’t seem like it’s any closer to resolution. It doesn’t seem like we are getting closer to peace in the world, instead it seems like we are getting further from peace. The Dalai Lama has done a lot of good work for peace in the world, but it’s sad that Tibet itself is very, very locked down.
Rigdzin: Yes, yes, very sad. Like I said, in the middle of night, 1 AM, 2 AM, your husband is gone, and nowhere to be found. And many years later, you learn, he was in prison and now he is dead. The dead bodies that’s all you can visit, it is very sad. But also, I’m sometimes more sad for Chinese officers who do that. They also have a family. Eventually, we have to look into our own eyes. We are our best witness. What did you do, right? What do you do wrong? We always say, “You are your best witness.” And, and there are many stories of the Chinese, that they are very sympathetic, that they’re completely lost in pain, coming in the middle of night to the Tibetan masters and asking for guidance.
DRK: Because they lose their humanity.
Rigdzin: Yes, they think they did it to Tibet, but the same thing happens to them. Somehow, human beings need to set a higher standard, like love, forgiving, equality. One person’s power is very dangerous. We have a saying, one person’s smartness is less than three mediocre people’s decision. The collective decision is better than one person’s decision. We always say that doesn’t matter how smart the individual is, the collective decision is better for everybody.
DRK: There’s the idea of engaged Buddhism, of religion or spiritual practice that is also a type of activism in the world. Thich Nhat Hanh, spoke of that, coming out of Vietnam. In what ways do you see Tibetan Buddhism, and your own life, as not a spiritual retreat from the world, but an engagement with the world.
Rigdzi: One hundred percent. Yes, one hundred percent. I think, of course, His Holiness Dalai Lama, and most Tibetan, for example, monks and nuns, begging to the Chinese officers and touching their shoes. They could have punched them. But those are examples of peace. You want peace, you want compassion, you want non-violence? They’re the examples. And it might take a long time. I really think that no, territory lasts forever. If you look, the Roman Empire, Hitler all gone. Soviet Union fell, right? So, change is imminent. A lot of Chinese are actually reclaiming their ancestors’ faith, which is Buddhism. So, China keeping Tibet is actually an asset for China and for the world. I sometimes say that Dalai Lama is begging China, okay, you can take Tibet as a part of China, but give us legitimate rights under your constitution, minority rights, religious rights, cultural practice, right? That’s all he’s asking. And if they give that to the Dalai Lama, and invite him back to Tibet, I think China will not become weaker, they will become more powerful. They will benefit from Tibet. But, Tibet will also contribute to the world as an example of non-violence and peace and harmony.
My dad, at that time, was very poor, in India. He talked a lot about Tibet having gold. I said, “Where is your gold, I am sick and tired of sitting in this tent!” And you know what he said? He said, “Oh, by the way, we don’t believe in digging for gold.” I said, “Why?” He said, “We are nomads, we’re farmers but also not only that, we are human beings. If you disturb mountains and rivers, the animals will suffer, whatever they eat will have a less nutrition.” That’s what he said. And now I think that is a big social ecology. But he didn’t have those fancy words. He was just saying, what do you drink, the vegetables you eat, and the sheep there, the grass they eat. Is it undisturbed? If the minerals are there, it has more nutrition. He said drinking milk in India, or drinking plain water in Tibet—the Tibetan water was more nutritious. That’s what he used to tell me.
Then I asked my father, “What do you miss the most about Tibet?” What they missed the most is the water of Tibet. When I went, I saw it coming right out of the glacier from the rock. It’s like a pain in your teeth—so, so cold—chilling—and oh so sweet. And now what China is doing, in my village, that same water they are bottling, without any blessing, they named it Tibetan Miracle Water. So, if you empty out all the rivers and all the water, then the largest population in the world, all of Asia will suffer. And also, there will be more earthquakes, because when you make dams like that, it changes the balance of the Earth.
TANTRA
DRK: Speaking of balance, what can you say about tantra?
Rigdzin: Tantra, I don’t know a lot, but yes, those are higher Buddhist view. In the ordinary view, we say this world is samsara. But, in tantra samsara is nirvana. Right? Samsara means that the world is contaminated, that it is delusion. Literally it means you are caught doing the same mistake over and over again—chaos, delusion, desire. Nirvana, that is the opposite, it means peace, equanimity. In tantra, one thing and its opposite can be seen as the same.
In tantra, you have to have a pure perception. Pure view means all sounds are mantras, Even if somebody says, “I hate you.” That sound is a mantra. All human beings are enlightened seeing things as pure. It is called Pure perception. So, then it is breaking into nondualism. So, there’s no dirty and clean. So having said that, we don’t teach tantra immediately because it can be misunderstood and someone thinks, okay, then you can kill a person. But as sometimes I say, clean and dirty, is a kind of superstition. It also means you’re stuck, it is a fixation on dualism. Tantra is about non-fixation, right? So, for example, sometimes this is a bad example. But when you make love, you put your mouth everywhere, whatever the sanitation is. But then in a restaurant you complain about a little bit of fingerprint on the glass and say it is a “dirty” glass.
So, tantra is like that, in some sense. I’m not talking about the sexual, but I’m, just reaching for an example, so the Western mind can understand.
Tantra is often not good to talk about because of the complexity. Sometimes we are just like kids, first you have to crawl, and then you start running, and then not only you start running, now you’re jumping in the air, leaping and you don’t get hurt, right? But the infant, if you throw in the air, they will get killed or die, right? So, if the tantra is heard at the right time, by the right person, it can be very profound. It is quick sweeping, like a highway, and makes faster awakening. But, without true understanding, it can be faster disaster. Ha ha ha!
Tantra, when done with the right kind of craziness does not create a mess in life. Actions have to be done with a kind of love, so that even if something is painful, it can still be nirvana.
DRK: In many religions, East and West, there seems like there’s often a focus on transcendence, moving from this world to some transcendent realm. Then there’s imminence, where the Divine comes down and infuses this world. And it seems like tantra focuses on both at the same time. It is not about getting away from this world, or beyond this world. And it’s not that the Divine is only in this world. It seems like there is a focus on imminence and transcendence at the same time—nonduality.
Rigdzin: 100% Yeah.
DRK: And the Native American and Indigenous religions they seem to have a very immanent focus, that the Divine is not separate from everything here—like you said about the Bon religion and the Nagas, it is in the water, the mountains, and all of life.
Rigdzin: So, that’s why most Buddhism has said that samsara is nirvana. In classic Buddhism, we divide into six different realms and some realms are unpleasant, like hell realm, hungry ghost realm. But my own interpretation is like in a chart where hell is equal to anger. When anger consumes, you create hell right now. Lust and greed create the hungry ghost realm, right now in the present. Extreme pride, ego is god realm. We can look at upper realms and lower realms as something out there, but we can experience, here, the whole six realms in one day. That’s why samsara and nirvana are right here, right now.
Do you have any more questions?
DRK: Yes, what about the concept of samvega that I asked you about earlier? That idea of experiencing dissatisfaction coupled with the desire to grow?
Rigdzin: Samvega, in my own interpretation, is, like, energy. You become fed up with the insubstantialness of our modern activities. Sometimes in Buddhism, we call it “wrong view,” wrong view will always lead you to pain and suffering. So, samvega, on other hand, is the conviction to break through this childishness.
Like, you said here, medical workers, they’re burnt out. But not all of them are burnout, right? It depends on how one looks at things. With samvega, you can tap into that energy, so that I at least have an opportunity to help. Sometimes you have to take the Buddha’s way of looking at tonglen or exchanging suffering and compassion. What if you are that sick person? That’s an even worse situation. Like if a sick person was dying. Would you rather die, or would you want to do anything? Like, sometimes, in my own experience, when I’m really sick, I wish I could just wash the dishes—that would be luxurious!
Sometimes you also get sick and you might suffer, but still, you are there voluntarily, and, also, fortunately helping the other. Right now, in this world, there are others who are doing similar service, but in freezing cold weather, and with not enough food to eat. But here, at least in America, you have a heater, you have hot running water, cold water, air conditioning, and a large dining room, and plus you get paid. I’m saying it’s always a matter of perspective. Perspective is a switch on and off our mind.
So yeah, we all need samvega, because now here’s a story. When I was the interpreter for Palden Gyatso, he said he got beaten every day. And sometimes they would hang him from the ceiling, and they put fire underneath him, like almost live barbecuing human being, but they burn enough to peel the skin, but not die, and then they beat him. And he said he used to think at the time, to overcome the pain and madness, of the 18th hell-ish realm, where the person who is punishing you, or burning you, or beating you, they don’t ever get tired in the hell realm. But, here, in this realm, the person beating me will definitely get tired in half an hour, then I will have some break. And then also, when he would get extremely mad at the person, he would think, if he doesn’t beat me, he’ll be beaten by the authority. So, that’s how he survived 33 years of torture, and when he came out, he was still sharp and razor clear in his mind. Not only that, other monks, including himself, when His Holiness gave them an audience and asked, “What was the scariest part?” And Garchen Rinpoche, whose life I know, he said, the scariest part was he was losing his vow of compassion to the enemy. So, these are some things we should cherish as human beings in this world instead of ignoring them and disregarding them. These are the pillars of path to peace.
TEACHING COMPASSION
DRK: How do you teach that kind of perspective? How do you teach compassion like that?
Rigdzin: The biggest issue is you have to always exchange places. Like, in the West, you say you have to put yourself in another’s shoes. In every aspect, not just torture, not just politics, even lust. They’re being taught as a monastic, that you have to think this is someone’s mother, someone’s sister, like that, right. And even that cannot sometimes put a stop to one’s own mind. So, you might have to analyze, if you imagine taking the skin off a person, they will be not desirable, right? If you look into the stomach, it’s not desirable. So of course, it’s very easy to say, but I’m saying, in every respect, we have some sort of exchange, equilibrium, and exchange oneself for the other.
Like if the Chinese person, whoever was beating Palden Gyatso, were to think for a moment, “What if I was that monk?” If even for a moment you have this genuine thought, you will be little bit hesitant to raise your hand. It is completely mad to see just yourself and not the other.
DRK: So, one way of teaching compassion is to exchange positions, to take somebody else’s perspective. You also talked about analytical meditation and meditating on death.
Rigdzin: With tonglen practice, sometimes you have to give all your merit, love, compassion, everything to the adversary and take all their pain and misunderstanding to yourself in visualization.
DRK: I think about what the heart does. For medical people, we know that the heart accepts the used-up blood, the blood that the oxygen has been taken out of, and the heart accepts it, and then the heart gives it away to the lungs. And then the lungs give the heart the richest blood, the most oxygenated blood, and then the heart accepts it, and then gives it away. So, the heart is this organ of giving and receiving and the organ of transformation of accepting both the bad and the good equally and giving them both away
Rigdzin: When you do this, when you exchange and take on other people’s pain, some people are able to but do this will not affect them. But at that time, when you do that, in my own experiences, when you do that, when it is a suffocating situation, disheartening, complete madness, it immediately gives a path, some kind of space. That’s my own experience. That’s why I’m saying our mind is limitless. It has no shape, no color.
When we talked about before tantra, Buddhists call, kha dhak [kadag], primordial perfection. We are all born with that, it never depreciates, it never needs any addition. It’s already there. The only thing is that we love to be deluding ourselves. We have the habit of falling into self-deception of samsara through our self-cherishing.
So how do you get a different vision in life? You have to act like a great meditator, even if you are not a great meditator, because you want to create that habit of exchanging oneself for another, taking everybody’s pain to yourself. Just like acting and then someday you realize that you’ve developed the habit. So, when somebody says, “Hey, I hate you,” you are more prepared to say oh, it’s just a word. He may be mad at someone else, maybe his coworker but he’s shouting at me.
BECOMING AN ARTIST
DRK: Let’s talk about art. When did you first think of yourself as an artist? What is the relationship between art and peace?
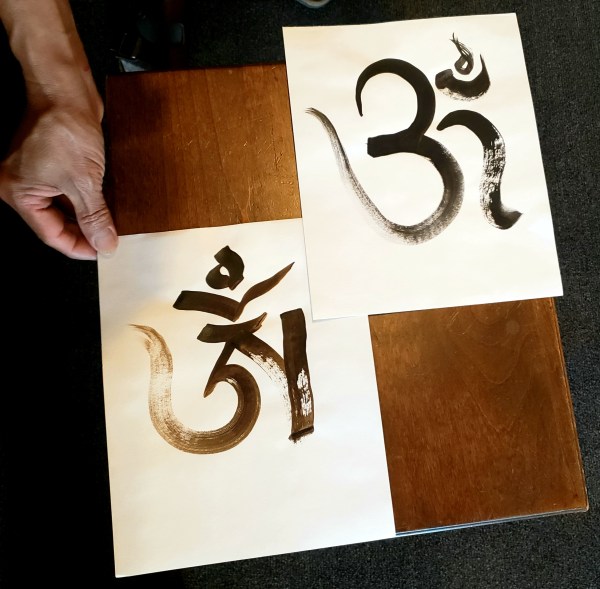
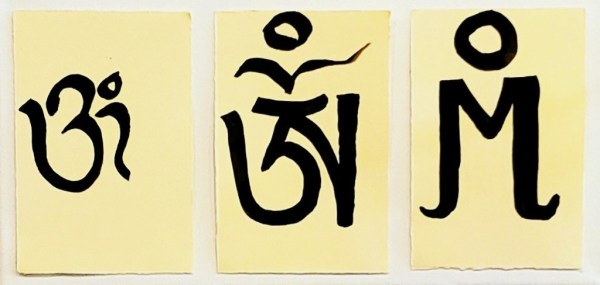
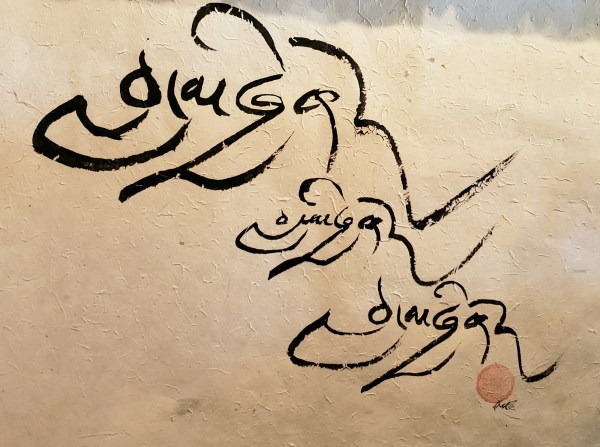
Rigdzin: I thought of art, at that time in childhood, as painting and coloring. I was having a hard time learning in school, especially different languages, like Hindi and English. And now I look at it, I actually have dyslexia. I see letters and numbers reversed. So, I always used to draw. Also it helped me with hunger. I get calmed down when I paint. I used to paint a lot of mountains and rivers. Maybe, in the back of my mind, I was missing those mountains and rivers, and tents and yak. That’s how my beginning was in art, but nowadays I do calligraphy.
When I was very young, in Dharamshala, when first at school, we didn’t have paper because we couldn’t afford it. So, we had to go to the jungle and cut wood. But sometimes we couldn’t even find wood properly. So, I remember sometimes we find bamboo bark. It’s very easy to clean. And then, the monks at that time, our teachers are all old monastery professors. But they are homeless. We are homeless—refugees. Yeah, so they’re our kindergarten teachers. So, they taught in old Tibetan monastic style. So, we had to bring any kind of flat slate or wood. Then, we’d go to our kitchen and and make a paste with the ashes and put on a slate. Actually, now I look back, and we made “dry erase,” but it was organic. And then monks will go and cut bamboo and flatten it. Then they teach alphabet, Tibetan alphabet, like a, b, c, d. So, then I learned to be really creative. In Tibetan, I write pretty well, compared to a lot of people. In Tibetan, we have three different styles of writing. One is newspaper writing, another one is big letter, and one is fast writing. So, sometimes I combine three in one in my calligraphy. So, it becomes very interesting. It will take a little while to read, but those who are good high school graduates, they can eventually figure out what that means. My calligraphy teaches about the Dharma in condensed form.
I think the Tibetan alphabet is one of the best languages to explore Buddha, Dharma, and the nature of the mind. Science researches the brain, but what about the mind? Tibetan culture and language has explored the mind and consciousness.
To end, I would like to speak about China. China has called the Dalai Lama a “wolf in monk’s robes.” They want the power and authority to choose the next, the 15th Dalai Lama, but His Holiness the 14th Dalai Lama has said that Dalai Lama will be born outside of China, in the West. He has said that if the Chinese really believe in reincarnation, they should be trying to find Chairman Mao’s reincarnation and leave the Dalai Lama to Tibetans. In his latest book, Voice for the Voiceless: Over Seven Decades of Struggle with China for My Land and My People, Dalai Lama says that the next Dalai Lama will be born outside of China as long as China occupies Tibet. Padmasabhava said in the 8th century that when the iron bird flies and the horses run on wheels, the teachings will leave Tibet and go to other lands and the Dharma will go to the land of the Red Men.
The ultimate teachings of Tibetan Buddhism are for achieving Naked Mind, pure consciousness for experiencing non-dualism. The teachings are that you should see the other as yourself, you should develop compassion for the other, that you should practice Samantabhadra to develop Universal Good for all sentient beings. Chöeying is the meaning of the innate nature of mind to experience dharmakaya, the ultimate body of truth. But really, it is simple, love everyone and every sentient being, exchange places with others to understand their suffering, and have compassion for everyone.
Pema Kharpo is located at 8554 Greenwood Ave N, Seattle, WA 98103
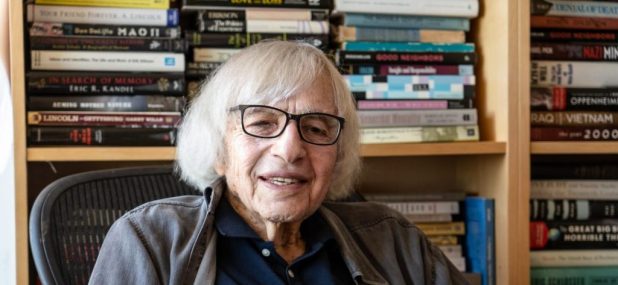
Robert Jay Lifton is an American psychiatrist and author whose subject has been holocaust, mass violence, and renewal in the 20th and 21st centuries. Lifton has written twenty-four books and edited eight others. His books include Death in Life: Survivors of Hiroshima (winner of a National Book Award); The Nazi Doctors: Medical Killing and the Psychology of Genocide (winner of a Los Angeles Times Book Prize); Home from the War: Learning from Vietnam Veterans; Thought Reform and the Psychology of Totalism: A Study of “Brainwashing” in China; The Protean Self: Human Resilience in an Age of Fragmentation; The Climate Swerve: Reflections on Mind, Hope, and Survival; and Witness to an Extreme Century: A Memoir.
He has been a leading public intellectual and antinuclear activist and is a founding member of the Nobel Prize winning International Physicians for the Prevention of Nuclear War. He has been a strong voice in opposing American wars in Vietnam, Iraq, and Afghanistan. More recently he has been active in the movement of psychological professionals to demonstrate the unfitness of Donald Trump for the presidency, and has written the foreword for the best-selling book The Dangerous Case of Donald Trump: 27 Psychiatrists and Mental Experts Assess a President (edited by Bandy Lee), and other articles on Trump’s dangerous psychological characteristics.
David R. Kopacz: I’d like to start by thanking you today for your time and tremendous body of work over the years. There are many ways that your work has influenced my work that I’d love to talk about, but I’m going to focus in, today, on the concept of the witnessing professional. I wonder if you could start by talking about this concept of the scholar-activist, the witnessing professional.
Robert Jay Lifton: I came to the idea of the witnessing professional in connection with a companion term of malignant normality. Malignant normality being the imposition on a society of a set of expectations that are highly destructive but are rendered ordinary and legal. Of course, the most grievous and extreme example of malignant normality is in connection with my work on Nazi doctors. In that sense, the German physician at the ramp in Auschwitz and other camps, sending Jews and others to their deaths was functioning in a kind of malignant normality. That is what he was supposed to do. That was his job, so to speak.
Within malignant normality we professionals have the capacity for exposing it, identifying it, and combating it, and that is the development or evolution of the witnessing professional. He or she is witness to the malignance of the claimed normality and not diminishing one’s professional knowledge but actually calling it forth as a means of creating one’s particular witness.
DRK: I wonder, how does this relate to our normal or historical concepts of professionalism, and how professionalism is taught today, in the health professions, with this tight focus on evidence-based medicine and protocols?
RJL: I became interested in the history of what we now call professionalism and the professions and, as you may know, it begins with profession as a profession of faith, of religious faith or commitment to a religious order. Over time, especially as we developed and moved into more of modern society, the idea of a profession became more associated with skills and increasingly technical skills. So, the idea of the professional or the profession became, what I would call technized, and the moral element of it was, in a sense, neglected or denied. In its most extreme form, the technized professional is a kind of hired gun for anybody who will pay him or her for professional knowledge. So, the witnessing professional, then, is a return to the inclusion of an ethical dimension in professional work. If you or I carry out some form of psychiatric or medical healing―that can be seen quite easily as a moral or ethical act. We shouldn’t lose the ethical dimension of being a professional. It is true that sometimes, as a professional, we have to step back and not experience fully another’s pain, or even the pain that we cause others, such as with a surgeon making a delicate operation or even a psychiatrist taking care of a very disturbed patient. But, at the same time we need to maintain, within the concept of the professional, that ethical or moral dimension and our own openness to some of that pain.
DRK: I am very interested in this idea of professionalism―in my writing I have contrasted the disconnection of the technician and the connection of the healer. I think this goes back, in a way, to the art and science of medicine. My first book was called Re-humanizing Medicine because I was concerned that people could develop that capacity―the psychic numbing or the splitting or selectiveprofessional numbing, which you write about―and that they would idealize that, and come to think that is what being a professional is: to be disconnected.
RJL: I think what you are referring to is the danger of what I call the technization of professions and considerable psychic numbing on the part of professionals, with diminished capacity or inclination for feeling―and that is dangerous. We see it is dangerous in different ways in every possible profession, I would say. So, in a way, the idea of the witnessing professional is an effort to recall a dimension of ethical involvement and limit psychic numbing on the part of professionals.
DRK: I suppose the difference is in being able to use psychic numbing as a conscious tool or technique rather than unconsciously assuming that identity of disconnection.
In thinking about the witnessing professional, there is often a narrative―and I just finished your autobiography, Witness to an Extreme Century―I’ve been really interested in reading the narratives of medical activists, people who take on this identity as a witnessing professional. The narrative goes, “I was minding my own business and just trying to be a good doctor when [X] happened, and I felt my training wasn’t adequate for [X], this experience in the world.” Is a witnessing professional―is it something that only happens in exceptional situations or is it something we can impart or teach to residents and students?
RJL: Yes, there are two questions there. One about exceptional situations and the other the capacity to teach residents or other young medical or psychological professionals the idea of the witnessing professional. A good example for me is the doctor’s antinuclear movement, which led to the formation of the International Physicians for the Prevention of Nuclear War, and perhaps you are referring to that. I have been quite active in it over the years and especially early on. What happened was, there was the capacity of first physicists, and then doctors in general, to recognize that they have something to say about nuclear danger. It began with the idea that doctors would be unable to carry out their traditional tasks in disaster, that is to help the living and provide some kind of healing. I used to talk and say the reason why this doesn’t work is because you’ll probably be dead, and we’ll probably be dead and there will be no medical facilities available for this. It is a recognition that one’s usual training can’t cover the extraordinary revolution in destructive weaponry that we’ve undergone and even the ethics of a particular profession are very inadequate because they would talk about being a kind therapist or bringing the latest knowledge to one’s work as a psychiatrist or physician but that’s not adequate for the problems that confront us. So, there can be these large threats, like nuclear threat, that awaken people to a realization that there needs to be a new, broader ethic that has to do with humanity in general.
All this can be taught, to a degree. One reason why the term ethical professional is useful is that it gives one a concept with which to connect one’s work and one can see oneself clearly as remaining a professional, not leaving the professional orbit, but using professional knowledge in a broader context. So, there can be lots of discussion and teaching and dialogue in relation to exactly this. It is already beginning to take place. You may know of a recent issue of Dædalus, which ordinarily is a highly professionalized journal, but they were able, they decided to devote one issue, which was edited by Nancy Rosenblum (who happens to be my partner), about witnessing professionals in relation to climate. I have an essay [“On Becoming Witnessing Professionals”] in it describing the witnessing professional which is the basis for the ideas of the issue. There always has to be a kind of development and commitment by individual people, and that development and commitment is enhanced by a collective expression of this kind of witnessing professional.
DRK: Thank you, I wasn’t aware of that issue. I will look that up. One thing I was wondering, in trying to teach this, how, how would you go about it? Is it a skill set that people can learn, that we can impart and measure? So much of medical education now is focused on objective learning goals. Or is it like a different dimension, like cultivating the heart and compassion and human connection. In other words, does one go into the work having been trained as a witnessing professional, or does one become a witnessing professional because one is open to human suffering and to look at that human suffering in a broader context than just being held within an individual in front of you in the clinic?
RJL: Well, it can be taught, what you are describing after all, with physicians in particular, is ostensibly a healing profession. A healing profession, or a professional who attempts to heal, has to take in pain and share the pain with patients, with others. Once one considers, early on, one’s work to be an ethical enterprise, it’s not too difficult for the witnessing professional to take root. I’ve mentioned in my work, observing very young physicians who were not clear about these matters, had some issues about them, but once they committed themselves to joining the physicians’ anti-nuclear movement, they themselves could evolve, become more articulate, and become more clear about who they were. In a strange way, I, in my own experience, as I think others did too, in the physicians’ anti-nuclear movement, felt myself more a healer than ever before in connection with this commitment. It is bound up with healing, for physicians. Of course, in my case, I had direct knowledge of the Hiroshima experience of people exposed to the first use an atomic weapon on a human population and what that caused and what that resulted in. I could talk about that, as together with Nagasaki, the only record we have of the human impact of, what is by present standards, a very small bomb. But even outside of what we consider directly healing professions, even professions that have to do with other forms of knowledge, including the humanities, can evoke their knowledge to confront the malignant normality that is put before us.
Of course, I’ve made use of the idea of malignant normality repeatedly and strongly in relation to Trump and Trumpism―it is not a single individual matter, but it is a collective form of behavior which pursues and seeks to render lying and deception and attacks, personal attacks on anyone who questions the “Big Lie,” render this the norm, the malignant normality of our own society and we are at the present time very much in the process of seeking to confront that malignant normality as witnessing professionals in our own society.
DRK: I’m glad you brought this up. You wrote the foreword [“Our Witness to Malignant Normality”] to The Dangerous Case of Donald Trump: 37 Psychiatrists and Mental Health Experts Assess the President. Like many people I was very concerned with, it seemed like many of the things that were happening were the things that happen in fascist or pre-fascist political movements. Dr. Bandy Lee brought that edited volume together, and brought you in for the foreword, and now she has been fired from Yale, ostensibly for violating the American Psychiatric Association’s Goldwater Rule. What are some of your thoughts on Bandy Lee’s work, her dismissal and also the warning this sends to professionals to “stay in your lane?”
RJL: Bandy Lee has been an extraordinary leader in speaking out about what I am calling malignant normality and encouraging psychological professionals to do the same. Nobody should be fired in relation to the Goldwater Rule, which is quite confused, and complicated with the resistance on the part of the American Psychiatric Association to a more thoughtful approach to psychiatrists speaking out, which could contain freedom to speak out while not making hands on diagnoses. I haven’t been working with Bandy Lee for several years and although the Goldwater Rule was mentioned by the Yale department, I am in no way clear about the whole Yale situation.
DRK: For myself, I went through this phase of feeling―“this is wrong, somebody should say something, somebody should do something.” I felt that collective psychology overlaps with my professional domain, and, additionally, I’ve also studied the literature outside of psychiatry, on fascism and history and the genocides of the last century. I felt a need to do something, on the one hand, but I wasn’t quite sure what to do. On the other hand, I had a fear of going beyond my profession if I were to speak out and point out similarities in current psychology to past fascist movements―and yet I was also aware of the “by-stander effect,” where people do not act when something is obviously wrong. I worry with Bandy Lee that this is a cautionary tale of―can you go too far as a witnessing professional, or is the ethical and moral right with the individual, even if they end up getting punished by the institutions?
RJL: What you are describing is a very human concern that witnessing professionals experience which has to do with how much one can say from the standpoint of one’s profession and how far one should go in saying it. There is, as you know, an interaction of psychology and politics that is inevitable. I think, in my own work, and there are others who do it a different way, I invoke what I know from professional experience, or what I think I know from professional experience, and bring it forward in relation to what I say publicly. In my case, of course, I’ve studied Hiroshima survivors and Nazi doctors and I’ve seen in the latter, in Nazi doctors, the very opposite of the witnessing professional. What I’ve called the “killing professional.” I think we have to speak out from what we have seen and recognized and then look at what we believe we know, or have learned, as a professional. Of course, in addition to that, we are also citizens who have ethical concerns about political issues. People have to give their own perspectives on this and there is no, how shall I say, there is no perfect model of how to go about it. But I think there is an increasing recognition on the part of many professionals that what they are doing and thinking is not enough and there is a hunger among professionals that I have encountered for entertaining or including an ethical or moral perspective in their professional work and I think that is increasingly available to people. So, yes, I believe that a witnessing professional should have discipline, one should say what one thinks one has learned as a professional, and not just speak randomly, and that’s really what defines the idea of the witnessing professional.
DRK: It feels like there is a sense in many witnessing professionals’ narratives of this being out on a limb by yourself, of not having been prepared by your education or profession, unless you have gone out of the way and read about different people who have taken on roles as witnessing professionals. So, I guess I go back again to this idea of―what would be the ideal way to teach this to medical students and residents and other health professionals?
RJL: I agree, it can and should be taught and should be discussed. You don’t have to have experienced an extreme situation in order to gravitate toward becoming a witnessing professional, after all, as you say, we undergo residency or training procedures of some kind and we experience all kinds of pain and have access to a lot of confusion on the part of both patient and healer. If we can look at a concept such as the witnessing professional that doesn’t automatically solve everything, but at least can provide a beginning in one’s sense of one’s self, one’s own identity as both a professional who is committed to learning, yes even the techniques of the profession, on the one hand, but is also committed to applying one’s professional knowledge in a broader way that enhances human behavior on a larger scale―that’s what the doctors anti-nuclear movement was about, there is also Physicians for Human Rights. These organizations then constitute a banding together of witnessing professionals who are always, or can always be, at the edge of activism.
The teaching that you emphasize, and discussion during residency, and even in medical school before that, I think could be very important. What happens, as you know, is that there is so much to learn in the training procedure that one is overwhelmed with memorization and details and the broader ethical dimension can readily be lost, but if it is considered early, it may never disappear entirely, and becomes part of, at least a possible, direction that starts early in psychological and medical professionals.
DRK: There are the studies that show that idealism goes down during medical student years and residency training and burnout starts to increase. I always wonder if somehow that idealism―maybe we should look at idealism as a precious resource rather than kind of a naïve, friendly fire incident with medical training where it is lost, where we could right from the very beginning come up with ways to help students preserve their idealism as they are learning that tight, technical focus to also be able to broaden out to the bigger picture.
RJL: Yes, what you say about idealism is important because, on the one hand, medical practice can be a business―it is in a way, but there is a certain element of idealism even a small one, that is likely to go into anyone’s decision to become a physician or a healer. As you say, it is readily lost in the training procedure which is demanding and dominates everything. If one can reconnect with the idealism, the earlier idealism, even a small element of it, that was a factor in that choice of profession, that could inform the witnessing professional. Or, to put it another way, if one has the concept of the witnessing professional that one has discussed early on in training, there is a place to recover and extend one’s idealism that is available in one’s mind because it has been placed there, as at least a possibility, early in one’s medical or psychological life. So, yes, in that way, the teaching of it, the discussion of it early would be very beneficial and students are very sensitive, as you know, and they are very responsive to what they perceive as authenticity and equally critical of what they perceive as less than authentic, the inauthentic. So, if the discussion is initiated with some sense of authenticity, coming from the experience of the initiator of the discussion, if he or she can tell about experiences that cry out for an element of idealism or of moral or ethical behavior in the professional, that will be responded to by students given their sensitivity and capacity to differentiate between what seems authentic to them or not.
DRK: I wonder whether we should institute practices, like some type of idealism practice and some type of suffering practice? A practice of being able to hold on to these ideals and recapture or regenerate them if they are lost. And a practice of being able to accept and embrace the suffering inherent in our professions and our work with people who are suffering and to be able to have a framework to metabolize and grow from that suffering―to turn the suffering into commitment to action in the world or re-dedication.
RJL: Yes, in recent work I have been talking about issues of death anxiety and death guilt and what I call an animating relationship to guilt or an animating relationship to death anxiety. These are forms of suffering which people we treat, or try to help, undergo and which we, ourselves, are hardly immune to and the animating relationship is the capacity to transform death anxiety or mea culpa guilt into what I call the anxiety of responsibility. The responsibility toward something in the way of healing or life-affirming behavior or contribution to the human future. So, these are very real matters. I think they are immediate and practical, but they are also very much aspects of what we call idealism.
DRK: I developed this idea of a counter-curriculum of re-humanization in medical school. I developed it in myself, by being connected to arts and poetry and literature and meditation, from a feeling that I needed to somehow push back against the ever-present scientific curriculum, to save some part of myself that was more than just memorizing biochemistry. I know you have written about the comparison between totalitarian thought reform and psychoanalytic training and I wonder if what is needed in medical education is some emphasis on this ability to be able to resist the brainwashing of technicism or thought reform of becoming an uncaring or unfeeling physician.
RJL: Well, there is a lot of pressure in medical training in the direction of psychic numbing, starting with the introduction to the cadaver. And I think that another way of saying what I think you are suggesting is that medical training involves diminution of feeling in the service of learning techniques.
Now, there is a reaction, getting to psychoanalysis―I’ve been in touch with some psychoanalytic groups in the last few years and there is a considerable movement away from the direction of totalism that I described which can inhabit psychoanalytic training, (which I myself partly underwent and then left). The American Psychoanalytic Association invited me to give their plenary address in 2020 and published it―a paper that specifically confronted thought reform and totalism. I talked about, in that plenary address, the imposition of ideas in a systematic way: criticism, self-criticism, and confession―which characterized Chinese thought reform and I talked about ways of avoiding this kind of totalism and combating it. The fact that I was invited to do so by the leading American Psychoanalytic Association suggests that they too are hungry for ethical directions. That doesn’t mean that much of medical or psychoanalytic training can still be questioned, but it does mean that there is a hunger for this broadening direction that I summarize in the form of witnessing professionals. I also talk about what I call the Protean style or capacity for individual change and transformation and that being associated with our tendency toward symbolism, not just one thing equals another, pen equal penis, or something like that, but rather a whole symbolizing tradition in philosophy and psychology, within which we must recreate everything we encounter, in order to take in anything at all. We are symbolizers, in that sense, and that opens us toward what I call a Protean Self or multiple Self. We have that capacity for combatting controls of the mind and we are also vulnerable to such a kind of process to a degree, but we also have inclinations within us toward rejecting it and opposing it―we can go either way.
I just learned that Robert Jay Lifton crossed over on September 4, 2025 – a few months ago. His books and work were a tremendous inspiration to me when I was in medical school and psychiatry residency. I was able to see him speak once, at the International Society for Traumatic Stress Studies annual meeting in New York City. I also interviewed him by phone 8/13/21, which can be found on The POV interview website that I run with my friend, Usha Akella.
I was particularly interested in his concepts of malignant normality and thewitnessing professional. Based on his work, as a social psychiatrist, interviewing Nazi doctors, atomic bomb survivors in Japan, and working with Vietnam veterans, Lifton went on to become a role model as a medical activist – speaking out about war, nuclear weapons, climate change, and late in his life, about the dangers of Donald J. Trump’s words and actions. Quotes below are from our interview.
“I came to the idea of the witnessing professional in connection with a companion term of malignant normality. Malignant normality being the imposition on a society of a set of expectations that are highly destructive but are rendered ordinary and legal. Of course, the most grievous and extreme example of malignant normality is in connection with my work on Nazi doctors. In that sense, the German physician at the ramp in Auschwitz and other camps, sending Jews and others to their deaths was functioning in a kind of malignant normality. That is what he was supposed to do. That was his job, so to speak.
Within malignant normality we professionals have the capacity for exposing it, identifying it, and combating it, and that is the development or evolution of the witnessing professional. He or she is witness to the malignance of the claimed normality and not diminishing one’s professional knowledge but actually calling it forth as a means of creating one’s particular witness.”
From his study of extreme socio-psychological situations, Lifton cautions us about the dangers of gradually growing to accept what is not normal – what he calls malignant normality. And he offers an antidote to malignant normality through the role of witnessing professionals whose ethics require us to speak up and speak out against social ills in the world – such as the climate crisis or American fascism and totalitarianism.
Lifton wrote the original foreword, “Our Witness to Malignant Normality,” for The Dangerous Case of Donald Trump: 37 Psychiatrists and Mental Health Experts Assess a President – Updated and Expanded with New Essays. Bandy X. Lee, psychiatrist and author of Violence: An Interdisciplinary Approach to Causes, Consequences, and Cures, brought together a group of civic-minded mental health professionals in 2017 for a conference at Yale, which was later published as The Dangerous Case, a first edition with 27 professionals, and later 37 professionals. Another trauma expert (another influence on my education in trauma and psychiatiry), Judith L. Herman, co-wrote the prologue with Bandy X. Lee, “Professions and Politics.”
Lifton’s concept of the witnessing professional provides a view of professionalism which moves beyond the narrow confines of the four walls of the consulting room to include the a responsibility to the larger ecological, social, and political world.
“I became interested in the history of what we now call professionalism and the professions and, as you may know, it begins with profession as a profession of faith, of religious faith or commitment to a religious order. Over time, especially as we developed and moved into more of modern society, the idea of a profession became more associated with skills and increasingly technical skills. So, the idea of the professional or the profession became, what I would call technized, and the moral element of it was, in a sense, neglected or denied. In its most extreme form, the technized professional is a kind of hired gun for anybody who will pay him or her for professional knowledge.
So, the witnessing professional, then, is a return to the inclusion of an ethical dimension in professional work. If you or I carry out some form of psychiatric or medical healing―that can be seen quite easily as a moral or ethical act. We shouldn’t lose the ethical dimension of being a professional. It is true that sometimes, as a professional, we have to step back and not experience fully another’s pain, or even the pain that we cause others, such as with a surgeon making a delicate operation or even a psychiatrist taking care of a very disturbed patient. But, at the same time we need to maintain, within the concept of the professional, that ethical or moral dimension and our own openness to some of that pain.”
Lifton’s work has inspired my own writing on the idea of medical activism as a professional, ethical responsibility, as well as my series of essays entitled Words Create Worlds.
Now, more than ever, we need to heed Lifton’s warnings about the risks of accepting malignant normality and we all need to embrace the idea of the witnessing professional.
For excellent overviews of his life’s work, see books:
Dave Kopacz & Chris Smith are joined founder and president of The Doctor as a Humanist – Jonathan McFarland. Chris joins us from a visit to the Driftless Area of Wisconsin (which Jonathan uses as a metaphor for a sense of loss of humanity in contemporary society – https://en.wikipedia.org/wiki/Driftless_Area), Dave speaks from his home in Seattle, and Jonathan joins from Mallorca, Spain.
Jonathan gives a brief history of himself as a human being, growing up in Liverpool, UK, surrounded by medicine and the arts. He describes how when his father, a surgeon, had a heart attack and was in the hospital, he had the idea of starting The Doctor as a Humanist (DASH). Jonathan has reached hundreds and thousands of students, educators, doctors, and other health care professionals through DASH. Jonathan clarifies that when he speaks of “doctors,” he means that broadly, to include all in health care – as doctor comes from the root docere, to teach.
We talk about what it means to be a humanist and why medicine needs re-humanizing. We jokingly define a humanist as someone who can’t answer a yes or no question without offering a quote from the arts or literature. They also speak of the possibility that when one is speaking of numbers and quantitative paradigms – the human is not present. Being a Humanist (and Becoming a True Human) are about values, compassion, and interpersonal connection.
Jonathan offers a definition of a humanist, “someone who cares about what is happening in the world around them and cares about the cultures” and the Earth. He touches upon the meanings of dignity and responsibility.
Jonathan mentions a book by Robert McFarlane, The Gift, which is “about the importance of giving books to others.”
We speak of and quote: John Berger, Bob Dylan, Martin Buber, Philip K. Dick, the Greek philosophers, Descartes, Spinoza, Gavin Francis, and many others.
Chris offers the quote from Buber, “All real living is meeting,” which feels like a good description of this incredible meeting between the three speakers today.
I’ve been thinking about how we need to build a community of practitioners discussing the problems of burnout, compassion fatigue, and soul loss. Isolation and loneliness contribute to burnout, and social connection is an antidote to burnout. To this end, we are creating the Becoming A True Human podcast. Who is “we”? Well, for now, it is me and my good friend Chris Smith – therapist, meditation teacher, Whole Health educator, storyteller, author (Be a Good Story), founder of the Academy for Mindfulness consulting, and all-around wise guy (and I mean that in multiple senses of the phrase).
The audio of the episode 1, Lost, is at the bottom of this post.
Chris SmithDave Kopacz
What is burnout? Just what exactly is it that burns out? How can whatever is burned out be re-ignited?
What is compassion fatigue? How does compassion wear out? Should it really be called empathy fatigue? Is the problem that there is too much compassion going out? Or not enough coming in? Or could it be that institutional structures and protocols make us busy with so many things that there is little time left in the clinical encounter for caring?
What is soul loss? Could we think of the soul being the “thing” that burns out? Not necessarily in a religious or metaphysical sense – although it could be if that fits your belief system – but in a metaphorical and psychological sense. If in burnout we lose connection with our souls, how can we reconnect and either go on a quest to find our lost souls, or create a welcoming environment in our bodies and lives so that our souls can return and flourish?
I address these questions in my book, Caring for Self & Others: Transforming Burnout, Compassion Fatigue, and Soul Loss, but we need to have further discussions around these topics as I feel strongly that we need a kind of ongoing practice, a yoga of burnout, in which we continually work in our own practices as well as in building communities of caring to support each other with this human, all too human dilemma.
Based on the topics we discussed in the first episode we titled this episode “Lost,” even before we realized that we somehow lost video of me and only recorded video for Chris! In this episode we explore topics of burnout as an initiation into becoming a wounded healer, soul loss, yoga for the health of healers, and we end with a meditation exercise and a poem, “Lost” by David Wagoner.
We don’t really know what we are doing with the technology aspect.
Let me tell you a story that illustrates the problem.
My high school friend Jack and I drove across the country after college. We were into the beat poets and writers, reading Kerouac’s On the Road, and envisoned a trip full of excitement and philosophical observations. We had a microcassette recorder and would talk into as we were driving, having many deep discussions and creating a record of what we saw.
Somewhere around South Dakota (having left from Chicago area) I noticed that the wheels of the recorder weren’t moving when we were recording. It was then that I noticed that there was a pause switch that was clicked on and prevented any recordings from being made! All of our bits, routines, observations, and experiences were lost! We were a bit crestfallen and we made half-hearted attempt to resume recording, but something had been lost – the energy, the enthusiasm. I think we eventually gave up on it. Maybe you could say we burned out on the idea after investing so much energy and enthusiasm and not having anything to show for it.
From a mindfulness perspective, there is surely some kind of lesson here – about not being attached to goals or outcomes, about being in the present moment versus memorializing experience, and maybe even that the organizing ego is an illusionary construct for creating a reduced and more manageable limited reality (if you want to take it that far!).
Well…I remembered this story after Chris Smith and I had just had our wide-ranging and enthusiastic discussion as we recoreded it on Zoom, only to realize that I had messed up the settings and we only had Chris’ video and both our audio. Well, crestfallen again! Urgh, technology failure again!
So, I think I have figured out how to share the audio of our video podcast, rather than have video of just Chris and my disembodied voice. Titling this episode, “Lost,” was prescient as we lost the video. Chris also spoke of his caring for self routine and how he purposefully skips some days so as not to get caught up in perfectionism, performance, and productivity. We’ll consider the lost video as a sacrifice to the Divine or the Cosmos, a giveaway, in addition to it being a bumbling failure of technology.
So, welcome to the first episode of the Becoming A True Human podcast – Lost – it highlights the vulnerability and imperfection of being human, that we are all a work in progress and that our work is a yoga practice – yoking mind, emotions, body, soul. The practice of Becoming A True Human is an ongoing practice, we can only do it in the present moment and the next moment we are again lost, at sea, trying to figure it out and Keep It All Together (KIAT). We will attempt to have the next episode as video and hope to post it on the Becoming a True Human YouTube site.
I’ve been doing a few podcasts lately – which is always a fun chance to talk about some of the work I have been doing. I’ll include a few photos from the past year to remind us of the world within which we all live & work.
Yellow Warbler in crab apple tree, Seattle, WA
I spoke with Andrea Nakayama on her 15-Minute Matrix Podcast on “Mapping the Costs of Caring,” looking at burnout, compassion fatigue, moral injury, and soul loss in health care workers. Here is an excerpt speaking about the similarities of burnout and soul loss:
The soul is the thing that makes us alive and vital and engaged and connected around the world. When we lose that, we lose all those kinds of things that connect us to ourselves and to others…How do we bring the soul back? It would be what things make the soul happy, what kinds of things bring you joy? And so how can you build this into your life? I think the distinction is you could start with self-care to support the ego, in the sense of your personality, but I think of the healer, the role of the healers, to be honest with delving into what can be the breakdown of the ego, and then the rebuilding back as a healer.
Yellow-Rumped Warbler in crab apple tree, Seattle, WA
I had a very nice dialogue with Lewis Mehl-Madrona and Glenn Aparicio Parry on his Circle of Original Thinking Podcast, “Integrating Healing Traditions with Lewis Mehl-Madrona and David Kopacz.” Definitely check this out, such an honor to have a generous time to speak with Lewis & Glenn. Check out their great books as well!
The print edition of Parabola Magazine, Fall 2023 featured “This Vibrating Land,” an excerpt from an interview that I did with Glenn Aparicio Parry that we featured on The POV interview website.
Perhaps burnout is a symptom of a larger problem. Perhaps we’ve cut ourselves off from a root of support in our work, we have lost touch with a spiritual and humanistic dimension of who we are and that when one suffers, all suffer. We have lost touch with our interconnection, our non-duality. What did Mother Teresa, Mahatma Gandhi, and Martin Luther King Jr. draw upon when working with the immense suffering in the world? Gandhi spoke of satyagraha as “the Force which is born of Truth and Love,” and Dr. King, spoke of this as “soul force.” Perhaps we should consider developing some kind of non-dual medicine, some kind of practice of non-separation in our healing work.
Last, but not least – I had a chance to catch up with former Seattle VA Primary Care Mental Health Integration teammate Dr. Nicola De Paul on “Burnout, Moral Injury, and Radical Caring” on her Menders: Love & Leadership in Health Systems Podcast. Check out our dialogue as well Nicola’s discussions with other great thinkers working to bring Love & Leadership into Health Systems!
If you have some down time, please check out any of these articles and podcasts that may be of interest to you, as well as look up some of the other great interviews on these podcasts!
“Healing is a very simple thing – all you do is stop separating things – on whatever level the separation is occuring. Whether it is you viewing your body as separate from your mind or your spirit being separate from your mind, or you viewing yourself as separate from nature.” (David Kopacz)
I agree with Marianela – that whenever we talk – we could go on for 3 days! Such an interesting and heart-warming conversation! You can watch the video of the interview here.
David R. Kopacz: I’d like to start by thanking you today for your time and tremendous body of work over the years. There are many ways that your work has influenced my work that I’d love to talk about, but I’m going to focus in, today, on the concept of the witnessing professional. I wonder if you could start by talking about this concept of the scholar-activist, the witnessing professional.
Robert Jay Lifton: I came to the idea of the witnessing professional in connection with a companion term of malignant normality. Malignant normality being the imposition on a society of a set of expectations that are highly destructive but are rendered ordinary and legal. Of course, the most grievous and extreme example of malignant normality is in connection with my work on Nazi doctors. In that sense, the German physician at the ramp in Auschwitz and other camps, sending Jews and others to their deaths was functioning in a kind of malignant normality. That is what he was supposed to do. That was his job, so to speak.
RJL: Within malignant normality we professionals have the capacity for exposing it, identifying it, and combating it, and that is the development or evolution of the witnessing professional. He or she is witness to the malignance of the claimed normality and not diminishing one’s professional knowledge but actually calling it forth as a means of creating one’s particular witness.
DRK: I wonder, how does this relate to our normal or historical concepts of professionalism, and how professionalism is taught today, in the health professions, with this tight focus on evidence-based medicine and protocols?
RJL: I became interested in the history of what we now call professionalism and the professions and, as you may know, it begins with profession as a profession of faith, of religious faith or commitment to a religious order. Over time, especially as we developed and moved into more of modern society, the idea of a profession became more associated with skills and increasingly technical skills. So, the idea of the professional or the profession became, what I would call technized, and the moral element of it was, in a sense, neglected or denied. In its most extreme form, the technized professional is a kind of hired gun for anybody who will pay him or her for professional knowledge. So, the witnessing professional, then, is a return to the inclusion of an ethical dimension in professional work. If you or I carry out some form of psychiatric or medical healing―that can be seen quite easily as a moral or ethical act. We shouldn’t lose the ethical dimension of being a professional. It is true that sometimes, as a professional, we have to step back and not experience fully another’s pain, or even the pain that we cause others, such as with a surgeon making a delicate operation or even a psychiatrist taking care of a very disturbed patient. But, at the same time we need to maintain, within the concept of the professional, that ethical or moral dimension and our own openness to some of that pain.
DRK: I am very interested in this idea of professionalism―in my writing I have contrasted the disconnection of the technician and the connection of the healer. I think this goes back, in a way, to the art and science of medicine. My first book was called Re-humanizing Medicine because I was concerned that people could develop that capacity―the psychic numbing or the splitting or selective professional numbing, which you write about―and that they would idealize that, and come to think that is what being a professional is: to be disconnected.
RJL: I think what you are referring to is the danger of what I call the technization of professions and considerable psychic numbing on the part of professionals, with diminished capacity or inclination for feeling―and that is dangerous. We see it is dangerous in different ways in every possible profession, I would say. So, in a way, the idea of the witnessing professional is an effort to recall a dimension of ethical involvement and limit psychic numbing on the part of professionals.
DRK: I suppose the difference is in being able to use psychic numbing as a conscious tool or technique rather than unconsciously assuming that identity of disconnection.
In thinking about the witnessing professional, there is often a narrative―and I just finished your autobiography, Witness to an Extreme Century―I’ve been really interested in reading the narratives of medical activists, people who take on this identity as a witnessing professional. The narrative goes, “I was minding my own business and just trying to be a good doctor when [X] happened, and I felt my training wasn’t adequate for [X], this experience in the world.” Is a witnessing professional―is it something that only happens in exceptional situations or is it something we can impart or teach to residents and students?
RJL: Yes, there are two questions there. One about exceptional situations and the other the capacity to teach residents or other young medical or psychological professionals the idea of the witnessing professional. A good example for me is the doctor’s antinuclear movement, which led to the formation of the International Physicians for the Prevention of Nuclear War, and perhaps you are referring to that. I have been quite active in it over the years and especially early on. What happened was, there was the capacity of first physicists, and then doctors in general, to recognize that they have something to say about nuclear danger. It began with the idea that doctors would be unable to carry out their traditional tasks in disaster, that is to help the living and provide some kind of healing. I used to talk and say the reason why this doesn’t work is because you’ll probably be dead, and we’ll probably be dead and there will be no medical facilities available for this. It is a recognition that one’s usual training can’t cover the extraordinary revolution in destructive weaponry that we’ve undergone and even the ethics of a particular profession are very inadequate because they would talk about being a kind therapist or bringing the latest knowledge to one’s work as a psychiatrist or physician but that’s not adequate for the problems that confront us. So, there can be these large threats, like nuclear threat, that awaken people to a realization that there needs to be a new, broader ethic that has to do with humanity in general.
RJL: All this can be taught, to a degree. One reason why the term ethical professional is useful is that it gives one a concept with which to connect one’s work and one can see oneself clearly as remaining a professional, not leaving the professional orbit, but using professional knowledge in a broader context.
So, there can be lots of discussion and teaching and dialogue in relation to exactly this. It is already beginning to take place. You may know of a recent issue of Dædalus, which ordinarily is a highly professionalized journal, but they were able, they decided to devote one issue, which was edited by Nancy Rosenblum (who happens to be my partner), about witnessing professionals in relation to climate. I have an essay [“On Becoming Witnessing Professionals”] in it describing the witnessing professional which is the basis for the ideas of the issue. There always has to be a kind of development and commitment by individual people, and that development and commitment is enhanced by a collective expression of this kind of witnessing professional.
DRK: Thank you, I wasn’t aware of that issue. I will look that up. One thing I was wondering, in trying to teach this, how, how would you go about it? Is it a skill set that people can learn, that we can impart and measure? So much of medical education now is focused on objective learning goals. Or is it like a different dimension, like cultivating the heart and compassion and human connection. In other words, does one go into the work having been trained as a witnessing professional, or does one become a witnessing professional because one is open to human suffering and to look at that human suffering in a broader context than just being held within an individual in front of you in the clinic?
RJL: Well, it can be taught, what you are describing after all, with physicians in particular, is ostensibly a healing profession.
RJL: A healing profession, or a professional who attempts to heal, has to take in pain and share the pain with patients, with others. Once one considers, early on, one’s work to be an ethical enterprise, it’s not too difficult for the witnessing professional to take root. I’ve mentioned in my work, observing very young physicians who were not clear about these matters, had some issues about them, but once they committed themselves to joining the physicians’ anti-nuclear movement, they themselves could evolve, become more articulate, and become more clear about who they were. In a strange way, I, in my own experience, as I think others did too, in the physicians’ anti-nuclear movement, felt myself more a healer than ever before in connection with this commitment. It is bound up with healing, for physicians.
Of course, in my case, I had direct knowledge of the Hiroshima experience of people exposed to the first use an atomic weapon on a human population and what that caused and what that resulted in. I could talk about that, as together with Nagasaki, the only record we have of the human impact of, what is by present standards, a very small bomb. But even outside of what we consider directly healing professions, even professions that have to do with other forms of knowledge, including the humanities, can evoke their knowledge to confront the malignant normality that is put before us.
Of course, I’ve made use of the idea of malignant normality repeatedly and strongly in relation to Trump and Trumpism―it is not a single individual matter, but it is a collective form of behavior which pursues and seeks to render lying and deception and attacks, personal attacks on anyone who questions the “Big Lie,” render this the norm, the malignant normality of our own society and we are at the present time very much in the process of seeking to confront that malignant normality as witnessing professionals in our own society.
DRK: I’m glad you brought this up. You wrote the foreword [“Our Witness to Malignant Normality”] to The Dangerous Case of Donald Trump: 37 Psychiatrists and Mental Health Experts Assess the President. Like many people I was very concerned with, it seemed like many of the things that were happening were the things that happen in fascist or pre-fascist political movements. Dr. Bandy Lee brought that edited volume together, and brought you in for the foreword, and now she has been fired from Yale, ostensibly for violating the American Psychiatric Association’s Goldwater Rule. What are some of your thoughts on Bandy Lee’s work, her dismissal and also the warning this sends to professionals to “stay in your lane?”
RJL: Bandy Lee has been an extraordinary leader in speaking out about what I am calling malignant normality and encouraging psychological professionals to do the same. Nobody should be fired in relation to the Goldwater Rule, which is quite confused, and complicated with the resistance on the part of the American Psychiatric Association to a more thoughtful approach to psychiatrists speaking out, which could contain freedom to speak out while not making hands on diagnoses. I haven’t been working with Bandy Lee for several years and although the Goldwater Rule was mentioned by the Yale department, I am in no way clear about the whole Yale situation.
DRK: For myself, I went through this phase of feeling―“this is wrong, somebody should say something, somebody should do something.” I felt that collective psychology overlaps with my professional domain, and, additionally, I’ve also studied the literature outside of psychiatry, on fascism and history and the genocides of the last century. I felt a need to do something, on the one hand, but I wasn’t quite sure what to do. On the other hand, I had a fear of going beyond my profession if I were to speak out and point out similarities in current psychology to past fascist movements―and yet I was also aware of the “by-stander effect,” where people do not act when something is obviously wrong. I worry with Bandy Lee that this is a cautionary tale of―can you go too far as a witnessing professional, or is the ethical and moral right with the individual, even if they end up getting punished by the institutions?
RJL: What you are describing is a very human concern that witnessing professionals experience which has to do with how much one can say from the standpoint of one’s profession and how far one should go in saying it. There is, as you know, an interaction of psychology and politics that is inevitable. I think, in my own work, and there are others who do it a different way, I invoke what I know from professional experience, or what I think I know from professional experience, and bring it forward in relation to what I say publicly. In my case, of course, I’ve studied Hiroshima survivors and Nazi doctors and I’ve seen in the latter, in Nazi doctors, the very opposite of the witnessing professional. What I’ve called the “killing professional.” I think we have to speak out from what we have seen and recognized and then look at what we believe we know, or have learned, as a professional. Of course, in addition to that, we are also citizens who have ethical concerns about political issues. People have to give their own perspectives on this and there is no, how shall I say, there is no perfect model of how to go about it.
RJL: But I think there is an increasing recognition on the part of many professionals that what they are doing and thinking is not enough and there is a hunger among professionals that I have encountered for entertaining or including an ethical or moral perspective in their professional work and I think that is increasingly available to people.
So, yes, I believe that a witnessing professional should have discipline, one should say what one thinks one has learned as a professional, and not just speak randomly, and that’s really what defines the idea of the witnessing professional.
DRK: It feels like there is a sense in many witnessing professionals’ narratives of this being out on a limb by yourself, of not having been prepared by your education or profession, unless you have gone out of the way and read about different people who have taken on roles as witnessing professionals. So, I guess I go back again to this idea of―what would be the ideal way to teach this to medical students and residents and other health professionals?
RJL: I agree, it can and should be taught and should be discussed. You don’t have to have experienced an extreme situation in order to gravitate toward becoming a witnessing professional, after all, as you say, we undergo residency or training procedures of some kind and we experience all kinds of pain and have access to a lot of confusion on the part of both patient and healer. If we can look at a concept such as the witnessing professional that doesn’t automatically solve everything, but at least can provide a beginning in one’s sense of one’s self, one’s own identity as both a professional who is committed to learning, yes even the techniques of the profession, on the one hand, but is also committed to applying one’s professional knowledge in a broader way that enhances human behavior on a larger scale―that’s what the doctors anti-nuclear movement was about, there is also Physicians for Human Rights. These organizations then constitute a banding together of witnessing professionals who are always, or can always be, at the edge of activism.
The teaching that you emphasize, and discussion during residency, and even in medical school before that, I think could be very important. What happens, as you know, is that there is so much to learn in the training procedure that one is overwhelmed with memorization and details and the broader ethical dimension can readily be lost, but if it is considered early, it may never disappear entirely, and becomes part of, at least a possible, direction that starts early in psychological and medical professionals.
DRK: There are the studies that show that idealism goes down during medical student years and residency training and burnout starts to increase. I always wonder if somehow that idealism―maybe we should look at idealism as a precious resource rather than kind of a naïve, friendly fire incident with medical training where it is lost, where we could right from the very beginning come up with ways to help students preserve their idealism as they are learning that tight, technical focus to also be able to broaden out to the bigger picture.
RJL: Yes, what you say about idealism is important because, on the one hand, medical practice can be a business―it is in a way, but there is a certain element of idealism even a small one, that is likely to go into anyone’s decision to become a physician or a healer. As you say, it is readily lost in the training procedure which is demanding and dominates everything. If one can reconnect with the idealism, the earlier idealism, even a small element of it, that was a factor in that choice of profession, that could inform the witnessing professional.
RJL: Or, to put it another way, if one has the concept of the witnessing professional that one has discussed early on in training, there is a place to recover and extend one’s idealism that is available in one’s mind because it has been placed there, as at least a possibility, early in one’s medical or psychological life.
So, yes, in that way, the teaching of it, the discussion of it early would be very beneficial and students are very sensitive, as you know, and they are very responsive to what they perceive as authenticity and equally critical of what they perceive as less than authentic, the inauthentic. So, if the discussion is initiated with some sense of authenticity, coming from the experience of the initiator of the discussion, if he or she can tell about experiences that cry out for an element of idealism or of moral or ethical behavior in the professional, that will be responded to by students given their sensitivity and capacity to differentiate between what seems authentic to them or not.
DRK: I wonder whether we should institute practices, like some type of idealism practice and some type of suffering practice? A practice of being able to hold on to these ideals and recapture or regenerate them if they are lost. And a practice of being able to accept and embrace the suffering inherent in our professions and our work with people who are suffering and to be able to have a framework to metabolize and grow from that suffering―to turn the suffering into commitment to action in the world or re-dedication.
RJL: Yes, in recent work I have been talking about issues of death anxiety and death guilt and what I call an animating relationship to guilt or an animating relationship to death anxiety. These are forms of suffering which people we treat, or try to help, undergo and which we, ourselves, are hardly immune to and the animating relationship is the capacity to transform death anxiety or mea culpa guilt into what I call the anxiety of responsibility. The responsibility toward something in the way of healing or life-affirming behavior or contribution to the human future. So, these are very real matters. I think they are immediate and practical, but they are also very much aspects of what we call idealism.
DRK: I developed this idea of a counter-curriculum of re-humanization in medical school. I developed it in myself, by being connected to arts and poetry and literature and meditation, from a feeling that I needed to somehow push back against the ever-present scientific curriculum, to save some part of myself that was more than just memorizing biochemistry. I know you have written about the comparison between totalitarian thought reform and psychoanalytic training and I wonder if what is needed in medical education is some emphasis on this ability to be able to resist the brainwashing of technicism or thought reform of becoming an uncaring or unfeeling physician.
RJL: Well, there is a lot of pressure in medical training in the direction of psychic numbing, starting with the introduction to the cadaver. And I think that another way of saying what I think you are suggesting is that medical training involves diminution of feeling in the service of learning techniques.
Now, there is a reaction, getting to psychoanalysis―I’ve been in touch with some psychoanalytic groups in the last few years and there is a considerable movement away from the direction of totalism that I described which can inhabit psychoanalytic training, (which I myself partly underwent and then left). The American Psychoanalytic Association invited me to give their plenary address in 2020 and published it―a paper that specifically confronted thought reform and totalism. I talked about, in that plenary address, the imposition of ideas in a systematic way: criticism, self-criticism, and confession―which characterized Chinese thought reform and I talked about ways of avoiding this kind of totalism and combating it. The fact that I was invited to do so by the leading American Psychoanalytic Association suggests that they too are hungry for ethical directions. That doesn’t mean that much of medical or psychoanalytic training can still be questioned, but it does mean that there is a hunger for this broadening direction that I summarize in the form of witnessing professionals. I also talk about what I call the Protean style or capacity for individual change and transformation and that being associated with our tendency toward symbolism, not just one thing equals another, pen equal penis, or something like that, but rather a whole symbolizing tradition in philosophy and psychology, within which we must recreate everything we encounter, in order to take in anything at all. We are symbolizers, in that sense, and that opens us toward what I call a Protean Self or multiple Self. We have that capacity for combatting controls of the mind and we are also vulnerable to such a kind of process to a degree, but we also have inclinations within us toward rejecting it and opposing it―we can go either way.
You can learn more about Robert Jay Lifton & his work at his website and his latest book, Losing Reality: On Cults, Cultism, and the Mindset of Political and Religious Zealotry is a summary of some of his most important books. This interview is also published at The-POV and is reprinted with permission.
Very grateful to my good friend, Dr. Carol Bowman for this interview with me and lively discussion on “Focus on What You CAN Do: Meaningful Engagement in Activities while Managing Chronic Pain,” focusing on the Personal Development circle of the Circle of Health as part of the VA Whole Health initiative from the VA Office of Patient Centered Care & Cultural Transformation. (Views are our own, although you can find it on the VA website).
My adaptation of the VA Circle of Health (I added the “We” to the center)
We talk about finding a place for pain in your life when you are working with chronic pain and different ways of transforming pain into compassion and personal growth.