Activism: A Foundational Element of Professional Identity
Over the past year I have been thinking about the idea of medical activism. I started drafting a paper and have wanted to pursue some of the sub-topics in greater depth and breadth, but I have lacked the time to put this together due to numerous other projects. Still, I believe that these ideas should be circulating at this particular time in history. I do not mean this as a definitive statement on medical activism, but rather I mean it to open a conversation.
Abstract:
The idea of medical activism has been criticized lately, from both inside[1] and outside[2] of the medical field. This paper takes the position that medical activism is a foundational element of professional identity – it defines who we are as professionals as opposed to being technicians or employees of institutions. Medical activism prioritizes caring and advocacy in the face of competing priorities of productivity and profit. Activism can take many forms, but its essence is when caring and healing extend beyond the internal biochemistry and inner thoughts of the client to include all the factors that we know influence individual and public health: childhood history, trauma, relationships, human rights, toxin exposures, environmental influences, and access to education and self-care. Two broad categories of medical activism are: 1) the reform of health care delivery systems, and 2) action in the political, cultural, legal, relational, and natural environments. These can also be conceptualized as internal (medicine in the clinic & hospital: having to do with the practice and delivery of health care) and external (medicine in the world: addressing public health issues outside the clinic or hospital). Examples of health care reform that will be considered are the movements of holistic and integrative medicine, Whole Health at the VA, the recovery movement in mental health, trauma-informed care, and addressing physician and health care worker burnout and suicide. Medical activism is born, again and again, when circumstances demand, from the identity of the physician/clinician as a professional and a moral agent in society whose “lane” is to treat disease, alleviate suffering, and to promote population health and well-being at local, national, and global levels. We need to make sure that the practice of medicine remains focused on healing and not just on making healthy profits or meeting institutional needs. Since the original conceptualization of this paper, new threats have arisen to the professionalism of medicine: fascism and political attacks on science. These political events, more than ever, remind us that if we do not use our voices we may lose them. Nourishing medical activism keeps the focus on care and compassion in health care and society. We must all adopt identities of what Parker Palmer calls “the new professional” and Robert Jay Lifton calls the “witnessing professional” in which we become moral agents within our world, tearing ourselves away from the never-ending demands of the Electronic Medical Records system, raising our gaze from the computer screen to the world we all live in.
Introduction:
The practice of medicine has changed greatly over the last 75 years, shifting from a practice of largely general practitioners who knew their patients over their whole lives to a fragmentation into sub-specialties, and the proliferation of multiple profit-deriving entities: the pharmaceutical industry, the insurance industry, and for-profit hospital and medical industry. During this time, doctors’ roles have shifted from independent healers engaged and embedded in communities to interchangeable and expendable bit-workers on ever more “efficient” medical assembly lines. Medicine has shifted from a focus on long-term healing relationships to a transactional, technician-based delivery system in which doctors are protocol-managers and data entry clerks.
The idea of medical activism encompasses the role of the physician as a moral agent, a member of a profession who answers to a higher calling. A professional has a moral calling that goes beyond the marketplace of the exchange of money or the influence of power. In speaking of medical activism, we wish to ground our discussion in the ancient profession of medicine, however we do also want to be inclusive and also use “medicine” in a larger context of health care professionals. The term, “healthcare activism,”[3] is a much larger term encompassing grass roots and activist/organizer movements. We do not mean to neglect this critical cultural force of health and healing, however for the purposes of this paper we are concerned with the identity of health care professionals as activists and medical activists.
In this paper we will develop the idea of medical activism as a form of moral agency which is a foundational element of professional identity. While there are many different forms of medical activism, we will focus on a few forms, such as, speaking out, bearing witness, critiquing systems and practices that contribute to disease and suffering, developing innovative delivery systems, reformulating philosophies of care and treatment, and advocacy to promote the health and well-being of individuals, local, national communities, and in this ever-more connected world, the global community. More recent public health issues have arisen with the Covid-19 coronavirus pandemic, the politicizing of sound public health measures (such as wearing masks and social distancing). Another growing public health concern is the growing fascist tendencies in the United States and abroad. We have a number of diagnostic manuals on fascism and we know that fascism is a public health issue: first it affects marginalized groups (Muslims, immigrants, Native Americans, African Americans, the LGBTQ community), then it affects those deemed dangerous to the regime (the “liberal” press, intellectuals, teachers, scientists, “liberal” politicians), and then it starts infecting more and more people with side effects of racism, xenophobia, hate speech toward the above groups, and eventually violence toward the above groups. To the end of cautioning the public about the public health risks of fascism, the formation of the professional organization, Doctors Against Fascism is proposed.
What it Means to be a Professional
To be a professional means that one is constantly professing – similarly if one is a profess-or. The roots of the word “profession” have to do with taking vows and declaring openly and to make public statement. The etymology of the word is related to “profess” and “prophet” going back to the ancient Proto-Indo-European root, *bha-, meaning “to speak, tell, say.”[4] What we are doing as professionals is continual professing – to declare openly and to speak, tell, say.
Our job as professionals it to profess, to declare openly, to speak, tell, say, to be prophets of health (which is different than focusing on the profits of the health care industry). The industry, the organization, the institution is not an inherently moral creation, it is more like a machine than a holder of morality, and it is the jobs of those professionals within the system to be the moral authority, the moral leadership of the institution.
De-professionalism
With the rise of economic and productivity medicine we have seen a deprofessionalization[5] and dehumanization[6] of physicians and health care professionals. Corporate medicine is not interested in moral agents or medical activists, but rather what Foucault called “docile bodies,” to play limited roles within the institution. Moral agents and medical activists function independently or semi-autonomously, rather than as interchangeable technicians who dispense the same, generic, non-individualized treatment interventions. While corporate medicine pushes propaganda of customer service, true caring, compassion, and patient-centered care can only be given by individuals to individuals in the context of human relationships. Individuality and humanity are extraneous and problematic variables to corporate, machine medicine.
Witnessing Professional
Throughout his career, Robert Jay Lifton has written about the idea of the witnessing professional. He describes the shift toward “malignant normality,” “the imposition of a norm of destructive or violent behavior, so that such behavior is expected or required of people”.[7]
As citizens, and especially as professionals, we need to bear witness to malignant normality and expose it. We then become what I call “witnessing professionals,” who draw upon their knowledge and experience to reveal the danger of that malignant normality and actively oppose it. That inevitably includes entering into social and political struggles against expressions of malignant normality.[8]
The New Professional
In order to teach the next generation of doctors, healers, and clinicians, we need to provide good role models for students to emulate. This is the transmission of knowledge and wisdom that happens from one generation to the next. Without medical professionalism, medical ethics, medical morals, students are left morally adrift. Author and educator, Parker Palmer speaks of the new professional, “a person who not only is competent in his or her discipline but also has the skill and the will to resist and help transform the institutional pathologies that threaten the profession’s highest standards.”[9]
Palmer states that “the very institutions in which we practice our crafts pose some of the gravest threats to professional standards and personal integrity. Yet higher education does little if anything, to prepare students to confront, challenge, and help change the institutional conditions under which they will soon be working.”[10]
“The notion of a ‘new professional’ revives the root meaning of the word. This person can say, ‘In the midst of the powerful force- field of institutional life, where so much conspires to compromise the core values of my work, I have found firm ground on which to stand―the ground of personal and professional identity and integrity―and from which I can call myself, my colleagues, and my profession back to our true mission.’”[11]
Science presents itself as “value-free” but the practice of medicine is one of moral agency.
Medical students enter the profession of medicine with idealism (which we know our medical education system diminishes) and yet they also enter having cultural biases. Research has been done on medical student attitudes toward homosexuality,[12] AIDS,[13] abortion,[14] the homeless,[15] immigrants,[16] and torture[17],[18] and how those attitudes might shape clinical care decision.
The Practice of Medicine as Continual Revolution & Reform
The beginning of Western Medicine is often said to have begun with Hippocrates who, rejected supernatural causes of illness, establishing the beginning of the scientific method and initiating a revolution of the truth which vanquished the other, competing, schools of medicine. The choice of Hippocrates as the “Father of Medicine” is somewhat arbitrary, as the study of nature, health, illness, and healing is ancient and has been practiced by all cultures. Hippocrates stands out as a medical activist in the musings of writers of history, as a medical activist championing science, rationalism, empiricism, and materialism.
The Structure of Scientific Revolutions
Thomas Kuhn, in The Structure of Scientific Revolutions, describes the stages of progress in science, starting with “normal science,” which mainly consists of technical puzzle solving. There comes a time when enough anomalies accumulate which do not fit the current scientific paradigm, which eventually leads to a crisis point. At the crisis point, the majority of scientists continue to adhere to a paradigm which is no longer as helpful as it once was, while a smaller group of scientists begin exploring new paradigms. Scientific revolution occurs when a new viable paradigm arises and there is conflict between the old and the new.
Semmelweis
Before the acceptance of germ theory, in the mid-1800s, Semmelweis tried to convince doctors that they should wash their hands after leaving off doing autopsies and before examining mothers who had just given birth. Although this seems common sense to us from our vantage point, Semmelweis was ridiculed, lost his appointment, and died in a mental institution. The concept of invisible pathogens was not part of the existing paradigm of understanding disease. We can consider Semmelweis as a medical activist who tried to protect the well-being of his patients and challenged the medical establishment.
Virchow
In the late 1800s, Virchow was tasked by the Prussian government to research an outbreak of typhus, in Upper Silesia, which had a large minority of Polish people living in poverty. His prescription was social and political: elimination of social inequality.[19] He came back with recommendations regarding poverty, services, and even political recommendations. This resulted in him losing his job. He wrote, “Medicine is a social science and politics is nothing more than medicine on a large scale,”[20] and that doctors “are the natural attorneys of the poor.”[21]
Social Determinants of Health
In addressing social determinants of health, Vicente Navarro writes that “we need to broaden health strategies to include political, social and cultural interventions that touch on the social (as distinct from the individual) determinants of health,” (15).[22]
Moral Determinants of Health
Berwick’s recent article, “The Moral Determinants of Health,” argues for an expansion of the role of professionals to include societal reform. “Healers are called to heal. When the fabric of communities upon which health depends is torn, then healers are called to mend it. The moral law within insists so.”[23]
Refounding: Reinvigorating the Founding Principles of Health Care
Another line of support for viewing medical activism as a core element of medical professionalism comes from anthropologist Gerald Arbuckle’s work on the concept of “refounding” in organizations. Arbuckle has observed that, over time, organizations and institutions lose touch with their original founding vision. A crisis-time comes and a “refounding individual” arises who challenges the status quo and seeks to revitalize the institution by bringing it back in line with the original, founding vision. The new state is a hybrid integration, though, of the new state of the surrounding culture and the original vision. This is to say it is not simply a return to the historic founding rules of the institution, but is a creative adaptation of the founding vision with a modern re-interpretation. An opposite way of trying to resolve the institutional crisis is a literal and rigid return to the past, which Arbuckle describes as the root of fundamentalism. Fundamentalism is reactionary and resists any change, growth, or adaptation. Refounding is a hybrid, bringing the spirit of the old into a new formulation within a new time and place. Arbuckle’s descriptions of the “refounding person” are consistent with the idea of the medical activist that we are discussing.
The ongoing health of institutions requires “refounding persons,” who remember the “original instructions” of the institution, the principles and ideals upon which the organization was founded but periodically loses its way. The refounding person is like the hero or heroine in Joseph Campbell’s hero’s journey – an individual who takes on what seems like an individual challenge that turns out to be healing for the entire community and places the people back in harmony with sacred and with the world. The refounding person is a person whose job it is to declare openly, to speak, say, tell, that we have lost our way, we have gone out of balance, and that we have to work to get ourselves back in balance, internally as individuals, in our relationships, in our community, and within our larger culture and our interrelationships with the world.
Cultural Models of Medicine within Contemporary Health Care
Interestingly, Arbuckle has worked in medical institutions as a consultant and this led to his book, Humanizing Healthcare Reforms. One of the challenges in healthcare reform, he finds, is that there are multiple cultures at play within modern medical settings and that in discussions between various clinical staff, accountants, and leadership, people bring different cultural world views, however these views are not clearly articulated and defined, so they are like invisible walls that impair discussion. He describes different cultural models of healthcare: traditional (indigenous medicine), foundational (Western values of care for the poor, sick, and suffering), biomedical (scientific, evidence-based medicine), social (living environment and inequalities), and economic rationalist (the business model of medicine with a focus on efficiency and productivity). These different cultural models of healthcare inevitably lead to cultural clash and crisis. Medical activism, or refounding, in healthcare would be a revitalization of some of the models of medicine (e.g. the traditional, foundational, and social) that have been neglected and suffered under the dominance of the economic rationalist and biomedical models. “In healthcare,” Arbuckle writes, “the need to refocus on moral and spiritual ideals means returning to a mission based on founding values such as solidarity, equity, respect and compassion,” (16).
Examples of Health Care Critique & Reform
An ongoing critique of the contemporary practice of medicine is a moral duty of physicians. It is up to us, as professionals, to hold true to the mission and purpose of health care: caring for people who are suffering and ill. Institutions may have vision and mission statements but they are incapable of moral agency and compassion because those are human traits, not bureaucratic functions. Within this critique of contemporary medicine, we will look at several issues: burnout, physician suicide, the pressure on physicians and health care workers to become narrowly defined technicians rather than healers, and the general loss of caring within the practice of health care.
Holistic and Integrative medicine are examples of reform and refounding. Many advocates of holistic and integrative medicine have felt corporate and biological reductionistic medicine have lost touch with the heart and soul of what it means to be a healer. The science of medicine has nearly eclipsed the art of medicine.
The following are some bullet points to be more fully developed:
- Limits of evidence-based medicine
- Groopman, How Doctors Think
- Beahr, The Limits of Scientific Psychiatry
- Pathological Objectivity
- Scientism – scientific fundamentalism
- As part of burnout triad – extreme form of emotional distancing
- Re-humanizing Medicine
- Counter-curriculum of re-humanization
- Holistic & Integrative Medicine
- Recovery Model in mental health
- Physicians for a National Health Program
- Micropractice, Ideal Medical Practice
- Work of L. Gordon Moore[24]
- Burnout
- Danielle Ofri: “The Business of Healthcare Depends on Exploiting Doctors and Nurses” [25]
- Physician suicide
- 300-400 suicides/year, size of three average medical school classes
Medicine in the World – Possible sections
The “first task of the doctor is therefore political: the struggle against disease must begin with a war against bad government,” (Foucault).[30]
Samuel Shem, in his essay, “Fiction as Resistance,” writes:
“We believed that if we saw an injustice, we could organize, take action, and change things for the better…When we entered our internship, we were told to treat our patients in ways that we didn’t think were humane. We ran smack into the conflict between the received wisdom of the medical system and the call of the human heart.”[31] Shem describes turning to fiction writing as a resistance to “brutality and inhumanity, to isolation and disconnection.” His recommendations on how to resist “the inhumanities in medicine” are four suggestions: 1) “Learn our trade, in the world” to be aware that “Medicine is part of life, not vice versa;” 2) “Beware of isolation. Isolation is deadly; connection heals;” 3) “Speak up…speaking up is essential for our survival as human beings;” 4) “Resist self-centeredness…learn empathy.”[32]
Bullet points to more fully develop examples:
- Human Rights
- Human Rights Medicine & Psychiatry, e.g. international trauma work
- Culture, Diversity, Religious Tolerance – addressing racism and intolerance
- Immigration policy and public health
- Judith Herman’s view of the tendency to forget trauma and the need to for those who work with traumatized populations to bear witness and be moral agents.
- Peace/Recovery from War & Violence
- The influence of Buddhism and Mindfulness in Health Care
- Preserving/Continuing Healing Traditions
- e.g. Shamanic work, physicians working with indigenous cultures who have written on benefits of incorporating elements into contemporary medicine
- Lewis Mehl-Madrona, in a study of Indigenous elders, learned that “Healers have to maintain some independence from political structures.”[33]
- Social, Climate, Environment
- Flint, Michigan – lead in drinking water
- Promoting the health of the Earth
A recent example of professional activism is found in the book, The Dangerous Case of Donald Trump: 37 Psychiatrists and Mental Health Experts assess the President. Many well-respected researchers and clinicians came together to raise awareness of public health and safety concerns stemming from their view of the dangerousness of the 45th president of the United States. Stephen Soldz and Brandy Lee write that
“Professionals are an important component…helping to provide checks on powerful institutions and alerting the public to wrongs. Professions operate with an implicit social contract with the broader society to contribute their special knowledge and training for the greater good.”[35]
They caution that what “is often missing from [ethics] training is any deep engagement with fundamental ethics principles and ethical thinking.” They see the comments and actions of the 45th President as a risk to public health and safety and feel that the safety risk comprises a duty to warn which overrides the past Goldwater rule which prohibits psychiatrists from diagnosing public figures.
They argue that the ethical principles of justice and universality “direct health professionals to pay attention to the wider world beyond the clinic as they call upon us to serve the broader public, not just those who become our patients. And they direct us toward the world of public policy and of ‘politics,’ broadly defined, as a way of collectively improving public health.”[36]
Soldz and Lee mention a number of recent examples of health professional activism, including opposing the involvement of psychologists and health professionals in torture under the Bush administration; opposing the use of psychiatrists in the Soviet Union to punish dissidents; physicians against nuclear war; physicians against land mines; and physicians supporting civil rights and health equity; and physicians for a national health plan.[37] They write that these examples illustrate that “activism by health providers is compatible with and even integral to professional responsibility toward society.”[38]
In this same volume, Robert Jay Lifton writes of the ideal of “witnessing professionals” who combine a “sense of outrage with a disciplined use of our professional knowledge and expertise.”[39] Lifton cautions that if we define ourselves too narrowly, as technicians, we lose our sense of identity as witnessing professionals. This is a caution alongside those who argue that many professions are being deprofessionalized.
- Doctors Against Fascism
- Proposed founding of this organization based on the systemic fascism in politics affecting public health
- Doctors as Public Health Advocates
- The Institute of Peace Medicine
I have long thought of writing a book called, Re-spiritualizing Medicine. This does not mean going backwards into religious fundamentalism, but rather recognizing that human beings are inherently spiritual creatures. By spirituality I do not mean religion, but rather a sense of aliveness, vitality, connection to other people, connection to the natural world, connection to something larger than our own egos. The spiritual underlies our sense of interconnectivity with humanity and all life.
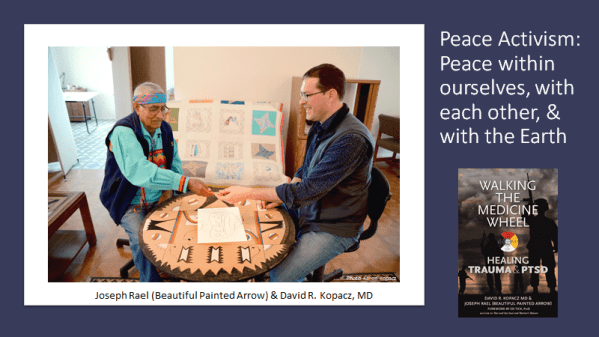
Since 2016 I have been working with Southern Ute visionary artist and healer, Joseph Rael (Beautiful Painted Arrow). His work since the 1980’s building Sound Peace Chambers around the world led to him being recognized by the United Nations for his work for world peace. Ultimately, peace is a public health issue, although we do not often think of it that way. War, violence, hatred, oppression, racism – all these are the opposite of peace. Perhaps we should found an Institute of Peace Medicine to address the social and moral determinants of health, but also to promote peace, unity, and non-duality as core human principles to protect and nurture human life and the life of the planet.
Spiritual Democracy
Joseph and I borrowed the term, spiritual democracy from Steven Herrmann. This idea of spiritual democracy also addresses many of the social and moral determinants of health. It also is an antidote to fascism. Fascism is founded on division and separation of us and them and on the priority of the will of the leader, and a small group of people defined to be like the leader, over the social good of the global community. Here is what Herrmann writes about spiritual democracy:
“Adopting the big idea of Spiritual Democracy, the realization of oneness of humanity with the universe and all its forces, can help people feel joy, peace, and interconnectedness on an individual basis. It can also inspire us to undertake sacred activism, the channeling of such forces into callings that are compassionate, just, and of equitable heart and conscience, and give us some tools to start solving some of these grave global problems, while uniting people on the planet.”[40]
Sacred Activism
The idea of spiritual democracy is related to the idea of sacred activism. This goes a step beyond professional or medical activism, but grows out of a common love and care for humanity and our environment. Herrmann credits Andrew Harvey for originating this term:
“Each of us, it seems, is guided by such a star and it varies in its fixed orbits, in different fields of sacred action, in every person’s life. A central existential task is to discover what that star is and to make its light, the inner fire of human love, burn brightly against the darkness, as a calling to live by. . . . Sacred activism is a spiritual practice for bringing about planetary changes through a receptivity to, and response to, experiences of a mysterious energy, force, or power, which move through the human body, psyche, and entire cosmos in an effort to bring about alterations of consciousness, cultural transformation, and ultimately: world peace.”[41]
World peace may seem like a big goal, but would that not bring about the greatest improvement in public, global health? The current US administration pulling out of the World Health Organization and the UN Human Rights Council is the opposite of what will heal us – as individuals, as communities, and as a stewards of the global ecosystem. Spiritual democracy, sacred activism, re-spiritualizing medicine and an Institute of Peace Medicine are logical extensions of the doctor and clinician as moral agents and profess-ors of public health.
Conclusion
We stand at a unique time in history – a global pandemic, smear campaigns against public health experts, attempts to silence or manipulate science for political ends, the politicization of basic, scientific principles of public health. We also stand at a time when fascist words are turning into fascist behaviors.[42] We have seen these early symptoms in the 20th Century and they can become fulminant and more deadly than a viral pandemic. Now, more than ever, we as physicians, we as clinicians, need to re-claim activism as a core identity. We need to speak, tell, say, to speak openly, to speak publicly about the public health threats of this time in history. We have guidance of those physicians and clinicians who have gone before us and how they have spoken up for the health of the people and the public.
We can draw on Robert Jay Lifton’s development of the witnessing professional. We can draw on Parker J. Palmer’s development of the new professional. We can draw on the moral foundations of our professions, to become moral agents for social change as we diagnosis and treat the moral determinants of health and the public health threats of the day.
[1] “Take Two Aspirin and Call Me by My Pronouns: At ‘woke’ medical schools, curricula are increasingly focused on social justice rather than treating illness,” Stanley Goldfarb, Wall Street Journal, 9/12/19
[2] “Doctors Revolt After N.R.A. Tells Them to ‘Stay in Their Lane’ on Gun Policy,” Matthew Haag, The New York Times, Nov. 13, 2018. The original criticism was in a Tweet from the NRA, “Someone should tell self-important anti-gun doctors to stay in their lane. Half of the articles in Annals of Internal Medicine are pushing for gun control. Most upsetting, however, the medical community seems to have consulted NO ONE but themselves.” https://twitter.com/NRA/status/1060256567914909702
[3] Laverack, Glenn. Health Activism: Foundations and Strategies. Sage: Thousand Oaks, 2013.
[4] Online Etymology Dictionary for “profession,” “profess,” “prophet.” https://www.etymonline.com/search?q=profession
[5] http://www.professionalsaustralia.org.au/blog/deprofessionalisation-matter/
[6] Kopacz, David. Re-humanizing Medicine: A Holistic Framework for Transforming Your Self, Your Practice, and the Culture of Medicine. Washington DC: Ayni Books, 2014.
[7] Lifton, Robert Jay. Losing Reality: On Cults, Cultism, and the Mindset of Political and Religious Zealotry. New York: The New Press, 2019, p. 189.
[8] Lifton, Robert Jay. Losing Reality: On Cults, Cultism, and the Mindset of Political and Religious Zealotry. New York: The New Press, 2019, p. 190.
[9] Palmer, Parker. The Courage to Teach: Exploring the Inner Landscape of a Teacher’s Life. San Francisco: Jossey-Bass, 2007, p. 202.
[10] Palmer, Parker. The Courage to Teach: Exploring the Inner Landscape of a Teacher’s Life. San Francisco: Jossey-Bass, 2007, p. 199.
[11] Palmer, Parker. “A New Professional: The Aims of Education Revisited.” Change, Vol. 39, No. 6 (Nov-Dec, 2007), pp. 6-12.
[12] Klamen, D, Grossman, L, and Kopacz, D. (1999). Medical student homophobia. Journal of Homosexuality, 37 (1): 53-63.
[13] Kopacz, D., Klamen, D., & Grossman, L. (1999). Medical students and AIDS: Knowledge, attitudes and implications for education. Health, Education & Research, 14 (1): 1-6.
[14] Klamen, D, Grossman, L, & Kopacz, D. (1996). Attitudes about abortion among second-year medical students. Medical Teacher, 18 (4): 345-346.
[15] Morrison, A., Roman, B. & Borges, N. Psychiatry and Emergency Medicine: Medical Student and Physician Attitudes Toward Homeless Persons. Acad Psychiatry 36,211–215 (2012) doi:10.1176/appi.ap.10080112
[16] Hudelson, P, Perron, NJ, & Perneger, TV. (2010). Measuring Physicians’ and Medical Students’ Attitudes Toward Caring for Immigrant Patients. Evaluation & the Health Professions, 33(4), 452–472. https://doi.org/10.1177/0163278710370157
[17] Dubin K, Milewski AR, Shin J, Kalman TP. Medical Students’ Attitudes toward Torture, Revisited. Health Hum Rights. 2017;19(2):265–277.
[18] Bean J, Ng D, Demirtas H, Guinan P. “Medical students’ attitudes toward torture,” Torture 18/2 (2008) pp. 99–103.
[19] Mackenbach, J. (2009). Politics is nothing but medicine at a larger scale: Reflections on public health’s biggest idea. Journal of Epidemiology and Community Health (1979-), 63(3), 181-184. Retrieved August 8, 2020, from http://www.jstor.org/stable/20720916
[20] Quoted in Vicente Navarro. What we mean by social determinants of health. Global Health Promotion Vol. 16 (1):5-16; 2009. Original reference: Virchow R. Die medizinische Reform, 2 in Henry Ernest Sigerist, Medicine and Human Welfare 1941:93.
[21] Mackenbach, J. (2009). Politics is nothing but medicine at a larger scale: Reflections on public health’s biggest idea. Journal of Epidemiology and Community Health (1979-), 63(3), 181-184. Retrieved August 8, 2020, from http://www.jstor.org/stable/20720916
[22] Vicente Navarro. What we mean by social determinants of health. Global Health Promotion Vol. 16 (1):5-16; 2009
[23] Berwick DM. The Moral Determinants of Health. JAMA. 2020;324(3):225–226. doi:10.1001/jama.2020.11129.
[24] L. Gordon Moore, ‘Going Solo: Making the Leap,’ Family Practice Management. February 2002, American Academy ofFamily Physicians website, accessed April 7, 2012.http://www.aafp.org/fpm/2002/0200/p29.html .
[25] Ofri D. The Business of Healthcare Depends on Exploiting Doctors and Nurses: One resource seems infinite and free: the professionalism of caregivers. The New York Times, June 8, 2019.
[26] Dean W, Talbot S, Dean A. Reframing clinician distress: Moral injury not burnout. [published correction appears in Fed Pract. 2019 Oct;36(10):447]. Fed Pract. 2019;36(9):400-402.
[27] Norman SB. Moral Injury. National Center for PTSD website. https://www.ptsd.va.gov/professional/treat/cooccurring/moral_injury.asp. Accessed April 27, 2020.
[28] ZDoggMD. It’s Not Burnout, It’s Moral Injury. March 18, 2019. https://zdoggmd.com/moral-injury/47 . Accessed July 30, 2020.
[29] Talbot SG, Dean W. Physicians aren’t ‘burning out.’ They’re suffering from moral injury. STAT. July 26, 2018. https://www.statnews.com/2018/07/26/physicians-not-burning-out-they-are-suffering-moral-injury/. Accessed July 30, 2020.
[30] Michel Foucault, The Birth of the Clinic (New York: Vintage Books, 1994), 38.
[31] Shem, Samuel. Fiction as Resistance. Annals of Internal Medicine. Vol 37(11):934-937; 2002.
[32] Shem, Samuel. Fiction as Resistance. Annals of Internal Medicine. Vol 37(11):934-937; 2002.
[33] Mehl-Madrona, L. “What Traditional Indigenous Elders Say About Cross-Cultural Mental Health Training,” Explore, 2009, 5:20-29.
[34] Michael H. Cohen, Healing at the Borderland of Medicine and Religion (Chapel Hill: University of North Carolina Press,2006), 3.
[35] Lee, Brandy X (ed). The Dangerous Case of Donald Trump: 37 Psychiatrists and Mental Health Experts Assess a President, Updated and Expanded with New Essays. New York: Thomas Dunne Books; 2019, p. xxviii.
[36] Lee, Brandy X (ed). The Dangerous Case of Donald Trump: 37 Psychiatrists and Mental Health Experts Assess a President, Updated and Expanded with New Essays. New York: Thomas Dunne Books; 2019, p. xxxi.
[37] Lee, Brandy X (ed). The Dangerous Case of Donald Trump: 37 Psychiatrists and Mental Health Experts Assess a President, Updated and Expanded with New Essays. New York: Thomas Dunne Books; 2019, p. xxxiv – xxxv.
[38] Lee, Brandy X (ed). The Dangerous Case of Donald Trump: 37 Psychiatrists and Mental Health Experts Assess a President, Updated and Expanded with New Essays. New York: Thomas Dunne Books; 2019, p. xxxv.
[39] Lee, Brandy X (ed). The Dangerous Case of Donald Trump: 37 Psychiatrists and Mental Health Experts Assess a President, Updated and Expanded with New Essays. New York: Thomas Dunne Books; 2019, p. xlix.
[40] Steven Herrmann, Spiritual Democracy: The Wisdom of Early American Visionaries for the Journey Forward, xiii.
[41] Herrmann, Spiritual Democracy, xvii–xviii.
[42] I have been writing a series of essay under the heading, “Words Create Worlds,” in the online magazine The Badger, https://beingfullyhuman.com/?s=words+create+worlds&submit=Search.